I recently recorded a podcast with Prof. Robert Hill and Richard Whatley (CEO at BioMin Technologies) on BioMin F toothpaste—an in-depth conversation on a very interesting toothpaste. During the preparation for this recording and after it, I developed an interest in the area as my understanding evolved. In this article, I wish to share my insight into some other considerations I have become aware of that we could include in building our understanding around toothpastes in general.
Over the past years, I have not really been drawn to analysing toothpastes to the extent that I have with BioMin F until the Oral Health Conference and Exhibition in Cardiff in the UK in 2019, when I came to learn about BioMin F, which made me want to explore toothpastes further.
As dental care professionals (DCPs), I and my peers have a duty to recommend toothpastes to our patients in alignment with supporting evidence. I would generally assess the patient’s overall needs, such as does he or she experience sensitivity, what is the trigger, are there any other relevant clinical conditions that I may need to take into consideration? On enquiring about what toothpaste he or she is currently using and identifying that the sensitivity is due to dentine exposure, I would follow on by checking whether his or her existing toothpaste aligns with his or her clinical needs and has supporting evidence, aligning with the recommendations outlined in Delivering BetterOral Health: An Evidence-Based Toolkit for Prevention.1 I would then share any information regarding any other options he or she could benefit from, for consideration in order to make an informed decision for change if required.
After running through my own personal assessment process of the questions I have surrounding toothpastes, I decided to reach out to a wider audience through social media, to understand what dental hygienists and dental therapists currently wish to know about a toothpaste to help build their understanding. I proceeded to pose a question on a social media platform for dental hygienists and dental therapists to gain a broader insight into what typical things we as DCPs look for in a toothpaste: “There is a new toothpaste on the market that is not specifically focused on treating anything in particular. What questions would you ask about the toothpaste?”
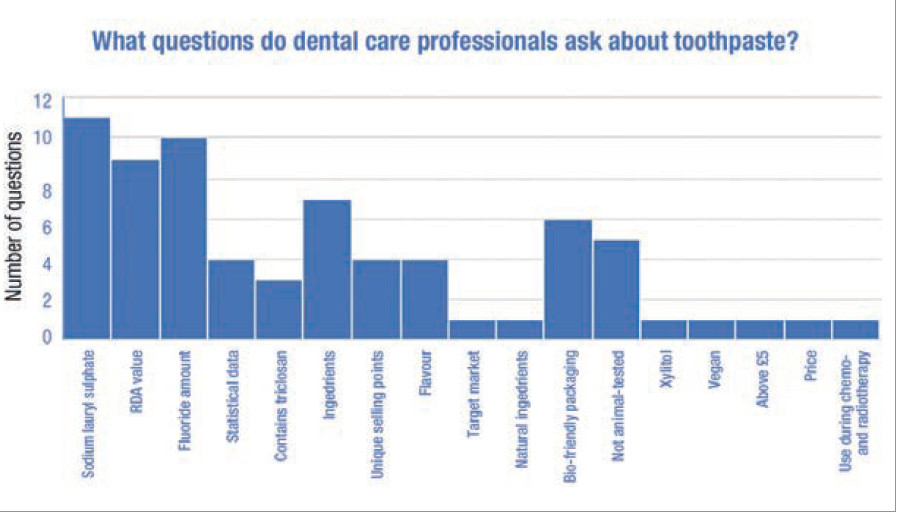
Fig. 1: Responses of 23 dental hygienists and dental therapists on features of dental toothpaste. RDA = relative dentine abrasion.
Figure 1 shows the responses of 23 dental hygienists and dental therapists obtained through the post on social media. Although this is a small group of respondents, these findings were interesting to understand what we as DCPs currently consider when we build our understanding of a toothpaste. The DCPs’ priority questions are as follows:
Does the toothpaste contain sodium lauryl sulphate (SLS)?
What is the toothpaste’s relative dentine abrasion (RDA) value?
What amount of fluoride does the toothpaste contain?
Why are we focused on SLS?
SLS and fluoride were certainly top of my list owing to the consensus that toothpaste containing SLS could contribute to aphthous ulcers. Yet, what is the evidence on SLS-containing toothpaste causing aphthous ulcers? According to a systematic review published in 2019, future well-designed trials are still required to strengthen the current body of evidence regarding recurrent aphthous stomatitis (RAS) and current evidence merely suggests that patients with RAS may benefit from using an SLS-free toothpaste.2 It appears that there is currently in sufficient evidence on the use of SLS toothpaste as a causative factor of RAS. Could this finding alter our thinking process in prioritising the need to know whether a toothpaste is SLS-free or not? If a patient shows signs of RAS, it would appear that we do not need to be recommending against the use of an SLS-free toothpaste linked to RAS. Even if a patient was to show signs of RAS, you could suggest stopping the SLS toothpaste for time, to monitor whether there is any change in the appearance of RAS, yet it may be questionable from the evidence to state that SLS is a causative factor.
Essentially SLS is a surfactant, which helps with the foaming and texture of the toothpaste. Surfactants are essential elements of toothpastes. A toothpaste being SLS-free does not necessarily mean that it is surfactant-free. It is the surfactants by nature that are slightly aggressive to soft tissue; swapping from an SLS-containing toothpaste to one containing an alternative surfactant does not necessarily overcome the RAS issue. Some surfactants are even more aggressive than SLS.
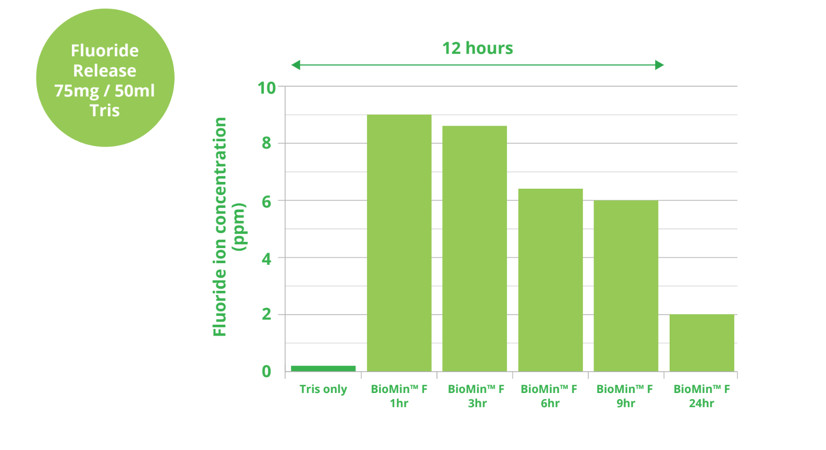
Fig. 2: BioMin F is a toothpaste containing glass materials that are able to dissolve slowly in saliva within 12 hours.
What is the evidence on fluoride?
There is sufficient evidence that supports the inclusion of fluoride in toothpaste. Relatively high-quality trials provide clear evidence that fluoride toothpastes are efficacious in preventing dental caries.3 An increased amount of fluoride in a toothpaste decreases the risk of caries, and in following Delivering Better Oral Health, which is evidence-based, we focus on the recommended amounts of 1,350 to 1,500 ppm fluoride.1
According to Prof. J.M. ten Cate, the world-renowned caries expert, “For treatments to be effective over periods longer than the brushing and the following salivary clearance, fluoride needs to be deposited and slowly released.”4 Research has shown that the quantity of fluoride is not the complete answer.
Considering Prof. Hill’s statements in the Smile Revolution podcast recording and what Prof. ten Cate has said, should we be questioning further the length of time the fluoride remains in the mouth, as well as the amount of fluoride and the mechanism by which the fluoride is made available in the mouth? For years, we have recommended a fluoride mouthwash in support of fluoride availability; however, if it is now possible for the fluoride to be released slowly over a period through a toothpaste, this could be optimal.
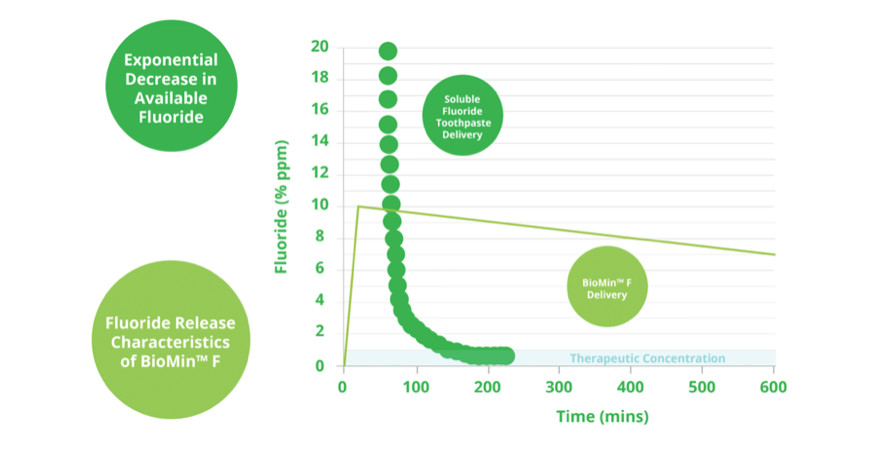
Fig. 3: BioMin F is a toothpaste containing glass materials that are able to dissolve slowly in saliva within 12 hours.
There is not enough fluoride in BioMin F, according to Delivering Better Oral Health. However according to Prof. Hill in the recent podcast recording, the toolkit was written prior to the release of BioMin F, so this could be a reason that the recommended fluoride content for children above seven, young adults and adults did not take into account the lower fluoride content of BioMin F. We will explore this further in the section on mechanism of bonding. The Oral Health Foundation however has accredited BioMin F as an approved oral healthcare product. The Oral Health Foundation evaluates consumer oral healthcare products to ensure that the claims made by manufacturers are clinically proven and not exaggerated.
RDA value
It is important to consider that tooth wear is multifactorial. The abrasiveness of the toothpaste will play a limited role in the overall process of tooth wear. From various articles, it would be fair to say that all toothpastes that have an RDA value of below 250 are considered safe to use. An RDA value of 250 or less produces little wear on dentine and virtually no wear on enamel for the long term if used with a correct brushing technique.7
Now that we have looked at the evidence supporting the most popular questions, I will look into our current understanding on the amount of fluoride in toothpastes in a bit more depth. Generally our questions are based on our knowledge; the greater our knowledge on a topic, the more questions we have in seeking to understand something further. Through recording the podcast with Prof. Hill and Mr Whatley, I learnt so much about BioMin F that my curiosity evolved around the additional benefits toothpaste could have in light of ongoing ingredient developments.
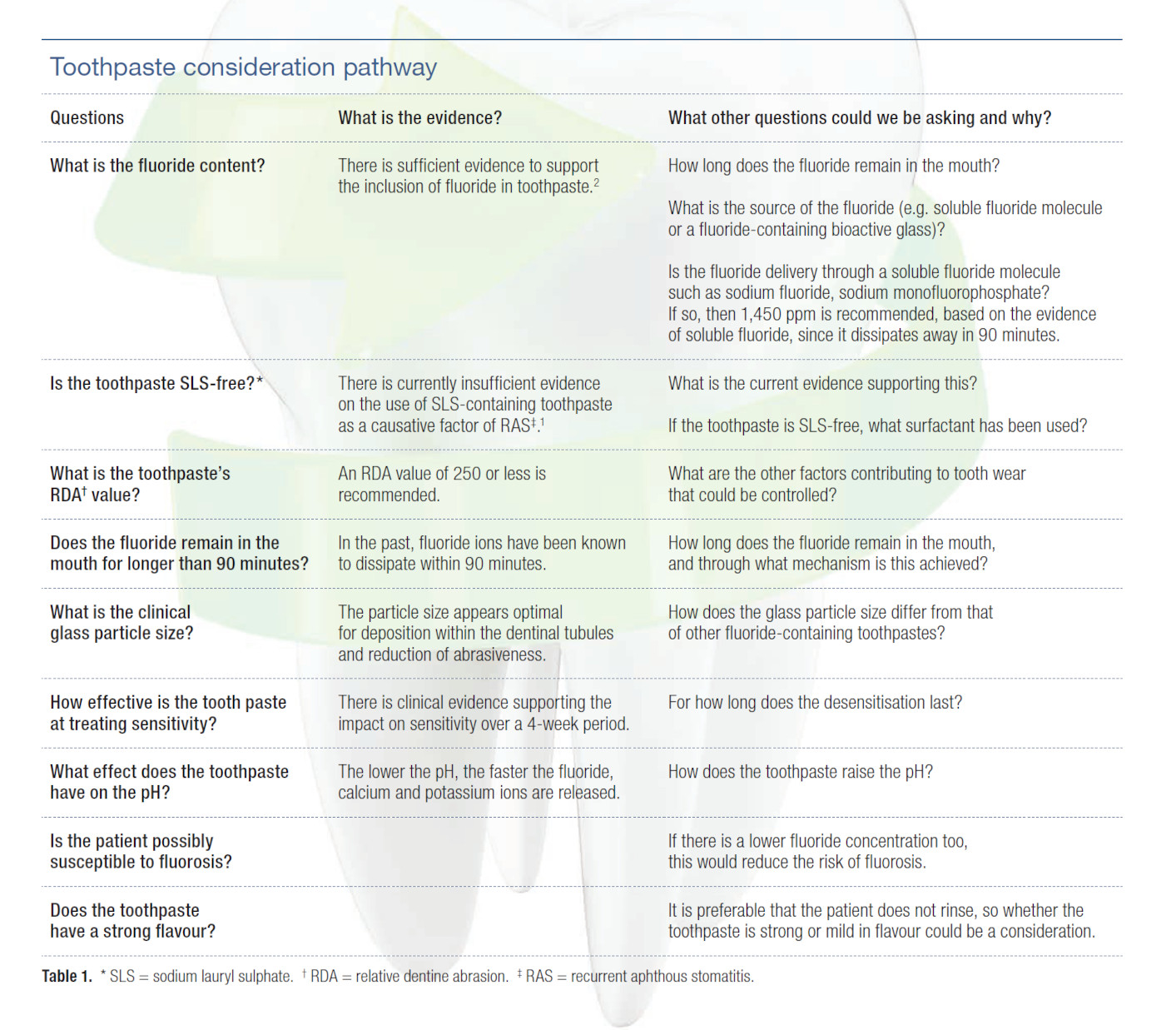
Through understanding the mechanism of BioMin F, I realized that this toothpaste could essentially become a significant contributing factor in the reduction of dental caries if used and recommended correctly. I have developed a pathway of questions that DCPs could utilise in evaluating toothpastes as part of future toothpaste analysis that have been inspired from the current questions and BioMin F (Table 1).
So what is different about BioMin F?
BioMin F is a toothpaste containing glass materials that are able to dissolve slowly in saliva within 12 hours (Figs. 2 & 3) and adhere to dental tissue. This is a particularly interesting, unique fact about BioMin F that aligns with what Prof. ten Cate has stated regarding the need for fluoride to be deposited and released slowly. There is only 600 ppm fluoride in BioMin F, the optimal amount of fluoride to exert a beneficial effect. Unlike other toothpastes,this is a favourable characteristic of BioMin F, especially for patients concerned about fluorosis.
Fig. 4: The mechanism of bonding of the glass particles to the tooth surface.
Although glass particles have been introduced into toothpaste previously, such as with NovaMin, which contains calcium and phosphate. The fluoride was not integrated into the glass particles. The concentration of phosphate in the glass particles of BioMin F toothpaste is much higher, accelerating apatite formation. As the glass particles dissolve, the ions are released, precipitating fluorapatite.
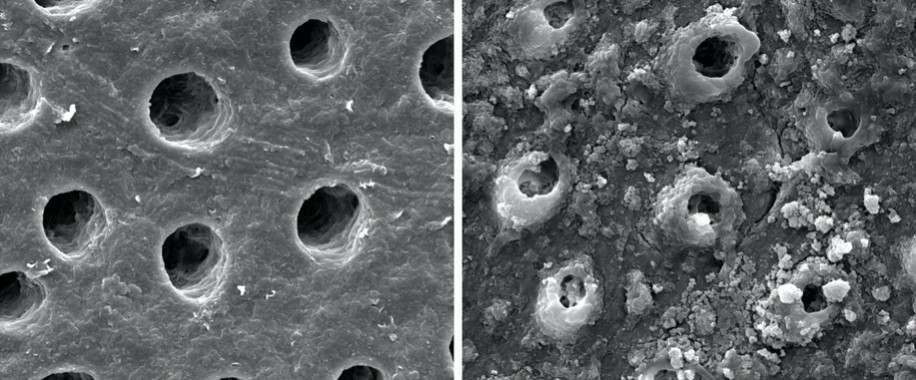
Fig. 5: The dentinal tubules before and after brushing with BioMin F.
In a comparative clinical study of 160 patients, the BioMin F group showed significantly better results compared with NovaMin, herbal and potassium nitrate toothpastes in the treatment of dentine hypersensitivity symptoms.5 Some clinicians have been reporting up to 90% relief from hypersensitivity. This is likely to be due to the size of the bioactive glass materials outlined in Figure 4. BioMin F has been developed to help reduce tooth sensitivity, and the size of the glass particle helps replace lost mineral from tooth surfaces to protect against acid erosion, as evident in the clinical trial. It is the particle size of the glass that helps reduce sensitivity through occluding the dentinal tubules as shown in Figure 5. The mechanism of bonding is perfectly shown in this image; it is important to remember that the glass particles adhere to tooth surfaces for up to 12 hours.
Fig. 6: How BioMin F works.
As with any toothpaste, there are external variables that could limit the toothpaste’s effectiveness however if the toothpaste is used twice a day and the patient does not rinse or eat directly thereafter then the toothpaste will be more effective. As Mr Whatley discusses in the podcast recording, it is also advisable for the patient to swirl the toothpaste around with his or her tongue to help distribute the toothpaste around the mouth.
How does the toothpaste react in a low-pH environment?
Bioactive glasses dissolve faster under acidic conditions than under neutral or basic conditions, quickly raising the pH and releasing calcium phosphate and fluoride ions; this is significant for caries-prone patients and patients who have a diet high in sugar. The fluorapatite dissolves at a pH value of just less than that of hydroxyapatite at 1.5 pH.
As a dental therapist and trained yoga teacher, Victoria Wilson certainly understands the holistic nature of oral health and overall well-being. In 2019, ...
SILVER SPRING, Md., U.S./LONDON, U.K.: BioMin Technologies has announced that its BioMin Restore Plus toothpaste has received 510(k) clearance from the Food...
Dentine sensitivity, causing discomfort and pain, particularly in reaction to hot or cold food or drinks, is a common problem. Mainly affecting people aged ...
Education
Live webinar Mon. 3 August 2026 8:00 pm EST (New York)

 Brazil / Brasil
Brazil / Brasil
 Canada / Canada
Canada / Canada
 Latin America / Latinoamérica
Latin America / Latinoamérica
 USA / USA
USA / USA
 Austria / Österreich
Austria / Österreich
 Bosnia and Herzegovina / Босна и Херцеговина
Bosnia and Herzegovina / Босна и Херцеговина
 Bulgaria / България
Bulgaria / България
 Croatia / Hrvatska
Croatia / Hrvatska
 Czech Republic & Slovakia / Česká republika & Slovensko
Czech Republic & Slovakia / Česká republika & Slovensko
 France / France
France / France
 Germany / Deutschland
Germany / Deutschland
 Greece / ΕΛΛΑΔΑ
Greece / ΕΛΛΑΔΑ
 Hungary / Hungary
Hungary / Hungary
 Italy / Italia
Italy / Italia
 Netherlands / Nederland
Netherlands / Nederland
 Nordic / Nordic
Nordic / Nordic
 Poland / Polska
Poland / Polska
 Portugal / Portugal
Portugal / Portugal
 Romania & Moldova / România & Moldova
Romania & Moldova / România & Moldova
 Slovenia / Slovenija
Slovenia / Slovenija
 Serbia & Montenegro / Србија и Црна Гора
Serbia & Montenegro / Србија и Црна Гора
 Spain / España
Spain / España
 Switzerland / Schweiz
Switzerland / Schweiz
 Turkey / Türkiye
Turkey / Türkiye
 UK & Ireland / UK & Ireland
UK & Ireland / UK & Ireland
 China / 中国
China / 中国
 India / भारत गणराज्य
India / भारत गणराज्य
 Pakistan / Pākistān
Pakistan / Pākistān
 Vietnam / Việt Nam
Vietnam / Việt Nam
 ASEAN / ASEAN
ASEAN / ASEAN
 Israel / מְדִינַת יִשְׂרָאֵל
Israel / מְדִינַת יִשְׂרָאֵל
 Algeria, Morocco & Tunisia / الجزائر والمغرب وتونس
Algeria, Morocco & Tunisia / الجزائر والمغرب وتونس
 Middle East / Middle East
Middle East / Middle East

 Dr. Cameron Shahbazian DMD MBARegister now1CELive webinar
Dr. Cameron Shahbazian DMD MBARegister now1CELive webinar
 Dr. Bruce McFarlane Certified Specialist in Orthodontics Fellow: Royal College of Dentists of Canada Diplomate: American Board of OrthodonticsLive webinar
Dr. Bruce McFarlane Certified Specialist in Orthodontics Fellow: Royal College of Dentists of Canada Diplomate: American Board of OrthodonticsLive webinar


 Prof. Dr. Wael Att, Dr. Andrea Laureti ITI Scholar Michigan, Dr. Acela MartinezLive webinar
Prof. Dr. Wael Att, Dr. Andrea Laureti ITI Scholar Michigan, Dr. Acela MartinezLive webinar
 Cat EdneyRegister now1CE
Cat EdneyRegister now1CE



















To post a reply please login or register