Population-wide databases for fingerprints6, 7 and DNA8, 9 are limited and very fragmented. After the 2004 tsunami disaster in Thailand, 46% of the victims were identified by dental records, compared with only 19% by DNA and 34% by fingerprints. The dental identification method is an analogous visual comparison of the ante mortem and post-mortem dental records.10, 11 The basis of this concept is that dental treatments are always very specific and unique.12, 13 To confuse matters somewhat, teeth are continually impacted by abrasion, disease, trauma and dental treatment. Thus, the available ante mortem data might not correlate well to the post-mortem data. Furthermore, treatment notation and information are not standardised, and it is exceedingly difficult to run an automatic search in a large, fragmented database.
Identifying the victim’s dentist, or, at the very least, the area where the victim was treated, is a mandatory prerequisite for a DVI search. Ante mortem dental records can be very challenging if no other victim information is available. In fact, younger patients may have only orthodontic records. The search process can be accelerated dramatically by accessing the ever-increasing number of digital scans and cloud-based data storage systems. Digital dental records must be retained, depending on national regulations, for years to decades.14, 15 Thus, digital dental records open new pathways for DVI. The logical next step is to determine oral cavity characteristics to employ that are universal, unique, invariable (stable throughout the life) and easy to access.
Monozygotic (MZ) twins cannot be distinguished by DNA analysis,16 and they look very similar (phenotypes). Hence, one way to prove the uniqueness of an identification method is its ability to reliably distinguish between MZ twins. It has recently been revealed that palatal morphology (palatal vault and surface texture) can differentiate MZ twins through intra-oral scans.17 Rugoscopy (also known as palatoscopy or calcorrugoscopy) is based on the difference in palatal rugae patterns and can distinguish among ethnic and race groups, offering great assistance during DVI.18–25 The palate is more resistant to burn deformation injury compared with the skin.26 It is stable over time and little varied after orthodontic treatment.27–30 The aim of this pilot study was to compare tooth and palate uniqueness using the intra-oral scans of MZ twins.
Methods
Three pairs of MZ twins, ages 17, 22 and 26, were enrolled in the study. The complete maxillary arch, including the palate, was scanned with the Emerald intra-oral scanner (Planmeca; software: Romexis Version 5.2.1). The palate was carefully isolated on each scan and was exported to a separate model. The left maxillary first molar was intact in five participants and filled in one participant. The left maxillary second molar was intact in each participant. These two teeth were segmented, and the images were exported to respective new files.
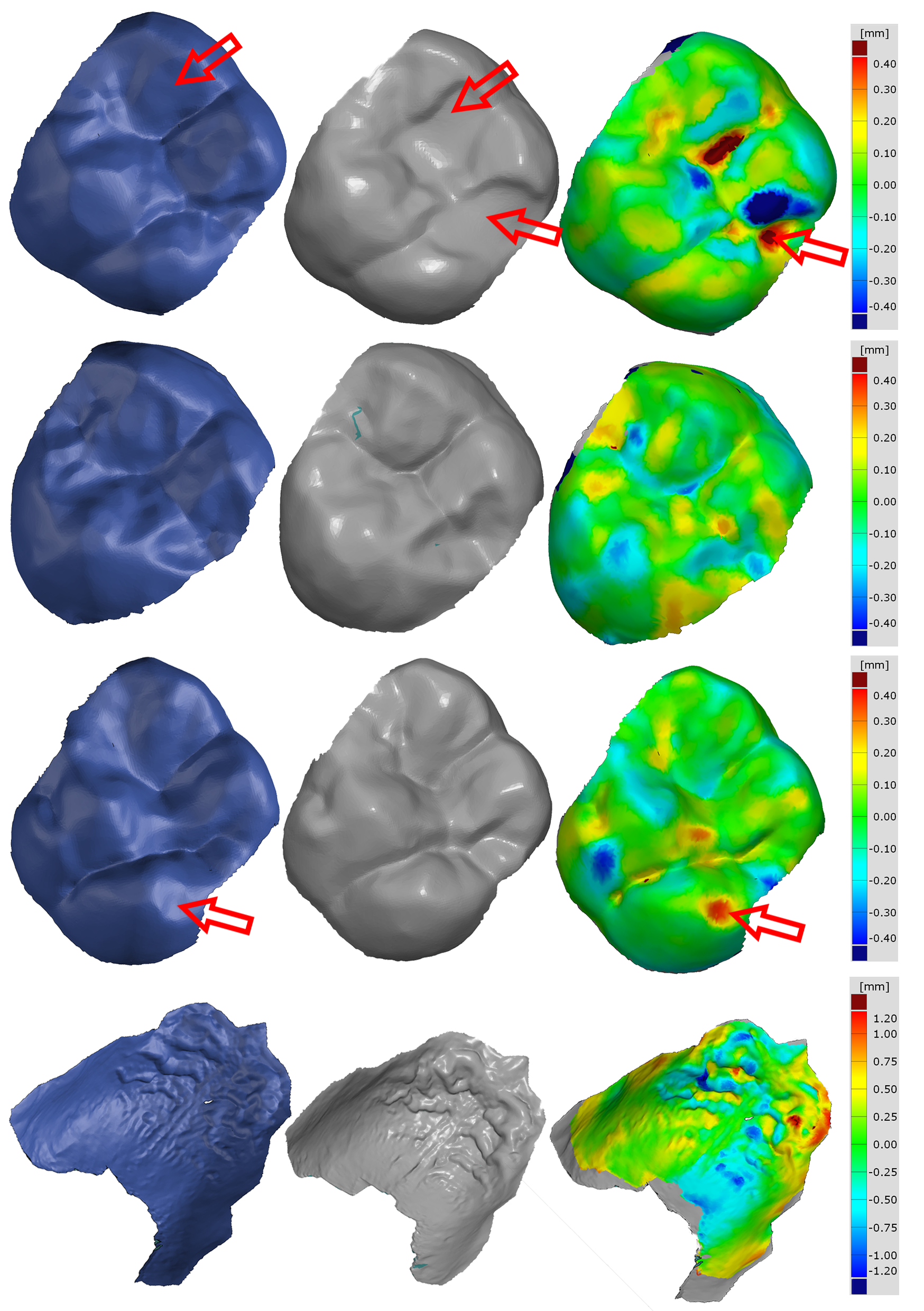
Figs. 2a–d: The digital casts of two siblings (grey and blue) and the surface comparison (colour map). Two maxillary first molars of the 22-year-old MZ pair (pair #3; a). The teeth had occlusal restorations, resulting in increased deviation (red arrows). Two maxillary second molars of pair #3 (b). These teeth had no restorations or abrasions. However, the occlusal surface morphology was quite different between siblings. Two maxillary first molars of 19-year-old MZ pairs (c). There were no restorations, and the cusp shapes were very similar. However, a sign of abrasion could be seen in the first sibling (blue), creating an increased deviation between scans (red arrows). The palate of pair #3 (d). The colour range in the palate was three times more than in the tooth map.
Digital palatal models and digital tooth models were aligned between non-relatives (Fig. 1) and between siblings. The superimpositions were made using the GOM Inspect software (GOM Metrology), utilising the local best-fit algorithm. The mean absolute deviations were calculated for each superimposition with the surface comparison tool. The data was statistically analysed by the generalised linear mixed model using SPSS (IBM SPSS Statistics for Windows, Version 27.0; IBM Corp.).
Results and discussion
The mean absolute deviations (± the standard deviation) of the first and second molars between non-relatives were not significantly different (0.259 ± 0.039 mm, 0.277 ± 0.037 mm; p = 0.733), but the mean absolute deviation of the palates was significantly higher (1.061 ± 0.314 mm; p < 0.001). Previous studies have found that a single tooth’s trueness is between 14 µm and 72 µm.31–33 The trueness of the palate has been reported to be between 80.5 μm and 130.5 μm.34, 35 Accordingly, the intra-oral scan can distinguish between unrelated people based on either tooth or palate imagery.
Molars in MZ siblings look very similar (Fig. 2). The mean absolute deviation of the first molars between siblings was significantly lower than the second molar deviation (0.087 ± 0.032 mm vs 0.137 ± 0.038 mm; p < 0.05). Notwithstanding that one of the first molars of the MZ pairs had restorations, these values were significantly (p < 0.001) lower than the deviations between non-relatives. Since these values are not much higher than the intra-oral scan trueness, they jeopardise the confidence in MZ twin identification. The palatal deviation between siblings was three to four times higher (0.393 ± 0.079 mm; p < 0.001) than the tooth deviation. Although, the deviation was significantly (p < 0.001) lower than the values between non-relatives, it was ten times higher than the precision (i.e. reproducibility, 35 µm) of a recent intra-oral scan.17 It was three times more than the trueness of the intra-oral scan regarding the palate.33, 34
Along with the present findings, there is increasing evidence that the 3D digital palatal model could serve as a highly reliable tool for human identification30, 36 and for distinguishing between MZ twins.17, 37 Recent and ongoing developments in intra-oral scanning technology will further improve the reliability. Digital casts of twins can also be used to study genetic and environmental factors in odontogenesis.38 It is of great importance that dentists should not discard digital models after completion of the dental work. These archived models are very useful for legal, forensic and rehabilitation purposes, now and far into the future.

 Brazil / Brasil
Brazil / Brasil
 Canada / Canada
Canada / Canada
 Latin America / Latinoamérica
Latin America / Latinoamérica
 USA / USA
USA / USA
 Austria / Österreich
Austria / Österreich
 Bosnia and Herzegovina / Босна и Херцеговина
Bosnia and Herzegovina / Босна и Херцеговина
 Bulgaria / България
Bulgaria / България
 Croatia / Hrvatska
Croatia / Hrvatska
 Czech Republic & Slovakia / Česká republika & Slovensko
Czech Republic & Slovakia / Česká republika & Slovensko
 France / France
France / France
 Germany / Deutschland
Germany / Deutschland
 Greece / ΕΛΛΑΔΑ
Greece / ΕΛΛΑΔΑ
 Hungary / Hungary
Hungary / Hungary
 Italy / Italia
Italy / Italia
 Netherlands / Nederland
Netherlands / Nederland
 Nordic / Nordic
Nordic / Nordic
 Poland / Polska
Poland / Polska
 Portugal / Portugal
Portugal / Portugal
 Romania & Moldova / România & Moldova
Romania & Moldova / România & Moldova
 Slovenia / Slovenija
Slovenia / Slovenija
 Serbia & Montenegro / Србија и Црна Гора
Serbia & Montenegro / Србија и Црна Гора
 Spain / España
Spain / España
 Switzerland / Schweiz
Switzerland / Schweiz
 Turkey / Türkiye
Turkey / Türkiye
 UK & Ireland / UK & Ireland
UK & Ireland / UK & Ireland
 China / 中国
China / 中国
 India / भारत गणराज्य
India / भारत गणराज्य
 Pakistan / Pākistān
Pakistan / Pākistān
 Vietnam / Việt Nam
Vietnam / Việt Nam
 ASEAN / ASEAN
ASEAN / ASEAN
 Israel / מְדִינַת יִשְׂרָאֵל
Israel / מְדִינַת יִשְׂרָאֵל
 Algeria, Morocco & Tunisia / الجزائر والمغرب وتونس
Algeria, Morocco & Tunisia / الجزائر والمغرب وتونس
 Middle East / Middle East
Middle East / Middle East


 Dr. Crystal Marruganti, Cat EdneyRegister now1CELive webinar
Dr. Crystal Marruganti, Cat EdneyRegister now1CELive webinar
 Federico ZunicaRegister now1CELive webinar
Federico ZunicaRegister now1CELive webinar
 Dr. Sergio FlorencioLive webinar
Dr. Sergio FlorencioLive webinar
 Dr. Cameron Shahbazian DMD MBARegister now1CE
Dr. Cameron Shahbazian DMD MBARegister now1CE



























To post a reply please login or register