Connected to a medical-grade vacuum at the top, the helmet would allow for containment of all droplets < 250 μm and 99.6% of all cough droplets overall. (Image: Dongjie Jia)
As part of work supported by a series of rapid-response grants for COVID-19-related research, mechanical engineering PhD student Dongjie Jia at Cornell University, U.S., helped develop a design for an open-faced helmet for patient use that is connected to a medical-grade air filtration pump from the top that creates a reverse flow of air to prevent cough droplets from entering the clinic environment. In an interview with Dental Tribune International, Jia explained how this project, which was funded by the Cornell Atkinson Center for Sustainability, was born and how it could help medical professionals in the ongoing pandemic.
Mr. Jia, how did you come up with the idea for the helmet, and how does it work? Our collaborators, Drs. Anais Rameau and Jonathan Lee Baker from Weill Cornell Medicine, came up with the original idea of a helmet. Dr. Mahdi Esmaily Moghadam suggested the nozzle design at the face opening to increase the reverse-flow region—the distance droplets need to travel against the flow before exiting the helmet—to increase droplet capture efficiency.
I drew the final prototype design using CAD. The working of the helmet is rather simple: The top tube is connected to a medical-grade vacuum, which potentially could be the same device that powers the saliva ejector. The vacuum will then create a reverse flow at the face opening to suck in the droplets ejected by the patient. According to our simulation, this device can contain all droplets < 250 μm and 99.6% of all cough droplets overall.
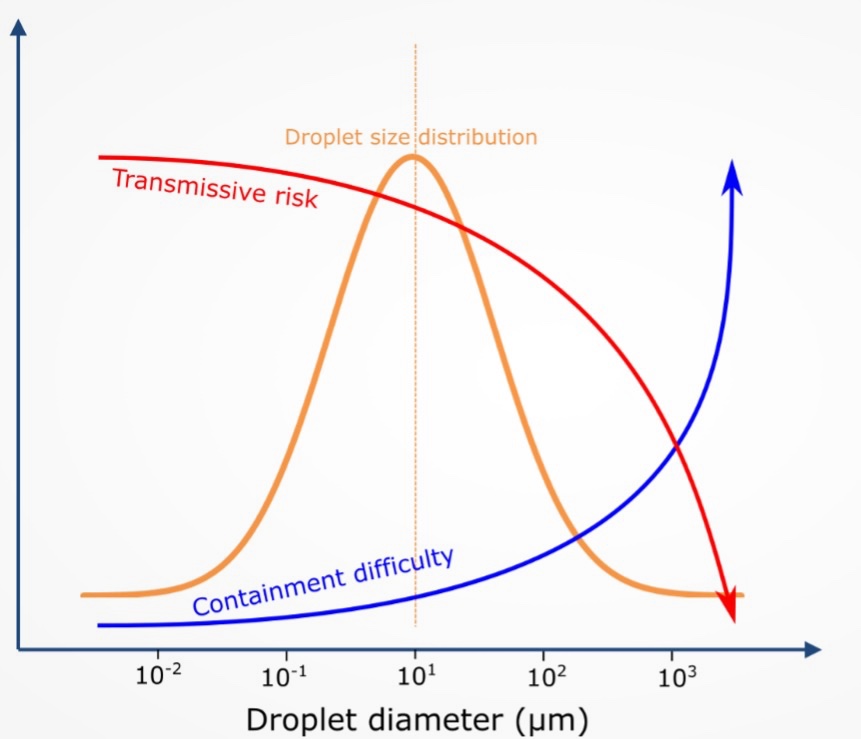
The reason larger droplets are harder to capture lies in the fluid dynamics of particles (droplets). In fluid dynamics, the particle relaxation time, which signals how quickly a particle adjusts to a change in flow, is a function of the particle diameter squared. Therefore, as the droplet’s diameter becomes larger, it becomes increasingly difficult to contain the droplet and for nozzle flow to influence it.
Larger droplets (> 100 μm) are less dangerous and less transmissive than smaller droplets are. Owing to their large mass, they tend to fall to the ground (or onto the face shield) within a second after they are released, whereas smaller droplets evaporate quickly and form much smaller droplet nuclei that stay in the air for hours or even days owing to their light weight. [This is demonstrated in the figure.]
Our design is extremely successful in capturing the more dangerous smaller droplets. The larger droplets that are not captured by our design can easily be delt with using face shields and practicing surface sanitation.
Owing to the nature of their work, dentists are particularly at risk of contracting SARS-CoV-2. What are the limitations of currently available personal protective equipment (PPE), and how could dentists benefit from using this device? The current PPE, such as N95 face masks and face shields, only protects dentists from infection, but it does not prevent patients from potentially contaminating the clinical environment. Cough droplets can remain airborne for hours after they are released. To deal with this problem, dentists typically need to have airborne isolation between patients and install expensive HEPA air filtration machines, which have a droplet removal efficiency of only around 90%. Our helmet can be made from disposable plastic and potentially cost around the same price as a face shield. Our device will provide a cheap and highly effective alternative.
What challenges has this project posed so far? The major challenge was to make sure that the simulation setup and results were accurate. The software we used has been rigorously tested for various flow situations. We also used analytical calculation to make sure our simulation result makes numerical sense. In the end, we are confident that our simulation closely resembles real-life situations.
What are the next stages in the research process? Are there plans to have the helmet manufactured and introduced to real-life clinical settings any time soon? Our collaborators are planning to prototype and test this device in clinical settings at Weill Cornell Medicine. If positive results are obtained in the prototype study, we may plan to contact manufacturers to produce this device for use in real-life clinical settings. Our current design is a proof of concept for the idea. We welcome any feedback from the clinical field to improve the ergonomics and practicality of our design.
Readers can learn more about the different droplet behaviors and classification in thefollowing here: Duguid JP. The size and the duration of air-carriage of respiratory droplets and droplet-nuclei. J Hyg (Lond). 1946 Sep;44(6):471–9. doi: 10.1017/s0022172400019288.
New research has explored how a miniature intra-oral robot could support more precise, more predictable and less invasive tooth preparation. The idea and ...
NEW YORK, US: Reduced salivary flow is a well-recognised feature of Down’s syndrome and is thought to contribute to the high prevalence of periodontal ...
TORONTO, Canada: The 19th MegaGen International Symposium, held in Toronto in June, focused on developments in implant dentistry over the past five decades....
COLOGNE, Germany: MegaGen, a global leader in dental implant innovation, continues to set new standards in implantology. MegaGen’s approach goes beyond ...
COLOGNE, Germany: As the name suggests, MegaGen’s AnyRidge implant system can be used for any implant case. Clinical results show that its benefits, ...
ZURICH, Switzerland: Global implant dentistry company Nobel Biocare has announced the first recipients of its newly established Medal of Excellence in ...
KLOTEN, Switzerland: Nobel Biocare has announced that it is adding the DEXIS Imprevo intra-oral scanner to its digital dentistry portfolio and distribution ...
Education
Live webinar Thu. 23 July 2026 2:00 pm EST (New York)

 Brazil / Brasil
Brazil / Brasil
 Canada / Canada
Canada / Canada
 Latin America / Latinoamérica
Latin America / Latinoamérica
 USA / USA
USA / USA
 Austria / Österreich
Austria / Österreich
 Bosnia and Herzegovina / Босна и Херцеговина
Bosnia and Herzegovina / Босна и Херцеговина
 Bulgaria / България
Bulgaria / България
 Croatia / Hrvatska
Croatia / Hrvatska
 Czech Republic & Slovakia / Česká republika & Slovensko
Czech Republic & Slovakia / Česká republika & Slovensko
 France / France
France / France
 Germany / Deutschland
Germany / Deutschland
 Greece / ΕΛΛΑΔΑ
Greece / ΕΛΛΑΔΑ
 Hungary / Hungary
Hungary / Hungary
 Italy / Italia
Italy / Italia
 Netherlands / Nederland
Netherlands / Nederland
 Nordic / Nordic
Nordic / Nordic
 Poland / Polska
Poland / Polska
 Portugal / Portugal
Portugal / Portugal
 Romania & Moldova / România & Moldova
Romania & Moldova / România & Moldova
 Slovenia / Slovenija
Slovenia / Slovenija
 Serbia & Montenegro / Србија и Црна Гора
Serbia & Montenegro / Србија и Црна Гора
 Spain / España
Spain / España
 Switzerland / Schweiz
Switzerland / Schweiz
 Turkey / Türkiye
Turkey / Türkiye
 UK & Ireland / UK & Ireland
UK & Ireland / UK & Ireland
 China / 中国
China / 中国
 India / भारत गणराज्य
India / भारत गणराज्य
 Pakistan / Pākistān
Pakistan / Pākistān
 Vietnam / Việt Nam
Vietnam / Việt Nam
 ASEAN / ASEAN
ASEAN / ASEAN
 Israel / מְדִינַת יִשְׂרָאֵל
Israel / מְדִינַת יִשְׂרָאֵל
 Algeria, Morocco & Tunisia / الجزائر والمغرب وتونس
Algeria, Morocco & Tunisia / الجزائر والمغرب وتونس
 Middle East / Middle East
Middle East / Middle East


 Dr. Crystal Marruganti, Cat EdneyRegister now1CELive webinar
Dr. Crystal Marruganti, Cat EdneyRegister now1CELive webinar
 Federico ZunicaRegister now1CELive webinar
Federico ZunicaRegister now1CELive webinar
 Dr. Sergio FlorencioLive webinar
Dr. Sergio FlorencioLive webinar
 Dr. Cameron Shahbazian DMD MBARegister now1CE
Dr. Cameron Shahbazian DMD MBARegister now1CE




















To post a reply please login or register