Although the final goal of the endodontic therapy is to provide symptom-free functional teeth with healthy periapical tissue long term,1 the severely damaged structure sometimes does not allow the clinician to succeed in the pursuit of saving natural teeth. In these scenarios, alternative treatments such as crown lengthening, autogenous transplantation or even implant placement should be considered with the objective of maintaining occlusal stability and functionality.2, 3
Autogenous transplantation refers to the repositioning of a tooth to another extraction site in the same patient; this can also apply to a tooth replanted into a surgically formed recipient site.4 In the past decades, the success rate reported for this procedure has increased in studies evaluation periodontal tissue healing and radicular resorption. The success rate reported in cases with complete root formation is 84%, and the success rate in teeth with non-complete root formation reaches 94%.5, 6 The most significant factor related to the success rate is the viability of the periodontal ligament attached to the root surface of the transplanted tooth; the viability of the periodontal membrane on the radicular surface will decrease after 18 minutes of extra-oral time.7, 8 This procedure tends to be technique-sensitive; operator skills and experience will play a crucial role in a successful outcome.
The transplanted tooth often presents with the crown structure totally intact. A large percentage of this cases will need root canal therapy; however, the removal of tooth structure needed for access cavity preparation and root canal shaping may undermine the strength of the tooth under functional load.9 Recently, conservative endodontic approaches have been recommended to minimise tooth structure removal and to preserve the very important peri-cervical dental tissue.
Among the different developments in dentistry that have made possible conservative approaches in endodontic practice are flexible endodontic files with controlled memory alloy and enhanced cyclic fatigue resistance, visual magnification, bioactive endodontic sealers, and sonic and ultrasonic irrigant activators.9–11 The development of these technologies has been crucial for making the conservative endodontic approach possible, prioritising the preservation of dentine, especially in the cervical region.12
Case report
A 16-year-old female patient was referred to the office for evaluation of tooth #16 (Fig. 1). The referring dentist asked that we apply all the available resources to save the tooth. The diagnosis was previously treated and symptomatic periapical periodontitis. After detailed examination, it was concluded that the tooth was not restorable. With the parents’ and patient’s agreement, we decided on an autogenous transplantation of tooth #18 to the site of tooth #16 after its extraction (Fig. 2). The orthodontist had determined that tooth #18 was to be extracted, and it was intended that the patient’s occlusion should be balanced by the end of the orthodontic treatment. Teeth #16 and 18 were extracted in the least traumatic way possible. After minor bone remodelling of the socket using low-speed burs, the third molar was transplanted to the recipient site (Fig. 3). A nylon monofilament flexible splint was used to keep the tooth in place (Fig. 4). Fifteen days later, the splint was removed, healthy soft tissue was observed, the patient was asymptomatic, and the tooth was stable in the site (Figs. 5a & b).
Fig. 1: Severely destroyed maxillary first molar with an old amalgam restoration, previous root canal therapy and recurrent caries.
Fig. 2: Periapical radiograph of the maxillary right molar. Tooth #18 was to be transplanted to the site occupied by tooth #16.
Fig. 3: Tooth #18 transplanted to
the site previously occupied by tooth #16.
Fig. 4: A nylon monofilament flexible splint was used to stabilise the transplanted
tooth in the recipient site.
Figs. 5a & b: Fifteen days post-op. Healthy periodontal tissue was evident around the transplanted tooth, before (a) and after (b) splint removal.
The original plan was to proceed with the root canal therapy three weeks after the replantation, but unfortunately, the patient did not attend the appointment. According to Tsukiboshi, it is not advisable to do the root canal therapy during the first two weeks, because of the risk of causing additional injury to the periodontal ligament, and it is advisable to proceed with the root canal therapy just after two weeks postoperatively in order to decrease the risk of inflammatory root resorption.6
The patient showed up to the clinic eight months later with signs and symptoms of pulp necrosis and acute periapical abscess; a periapical radiolucency was present, and the retromolar area was healed (Fig. 6). In cases like this, where the coronal structure remains intact, it is advisable to take a conservative approach to the root canal therapy, using new technology available in endodontics to achieve good results. The endodontic access opening was created using high-speed burs and ultrasonic tips. The cleaning and shaping protocol was performed with flexible needles and controlled memory files (Aurum Blue, Meta Biomed), especially important properties for entry to the root canals through the conservative access (Figs. 7a & b).
Fig. 6:
Eight-month post-op radiograph. The retromolar area had healed, but the transplanted tooth showed signs of pulp necrosis and periapical disease.
Figs. 7a & b: Clinical photographs of the tooth just before initiating the root canal therapy (a) and just after nishing the endodontic access opening (b).
Figs. 8a–c: Root canal entrances obturated and pulp chamber oor cleaned palatal (a), mesiobuccal (b) and distobuccal (c).
Fig. 9: Final radiograph of the root canal therapy and coronal restoration. Placing the coronal filling material into the pulp chamber tends to be complex with such a small access opening.
Figs. 10a & b: Adhesive coronal restoration, just before (a) and after (b) removal of the isolation.
Fig. 11: Three-year follow-up radiograph. The periapical area had healed.
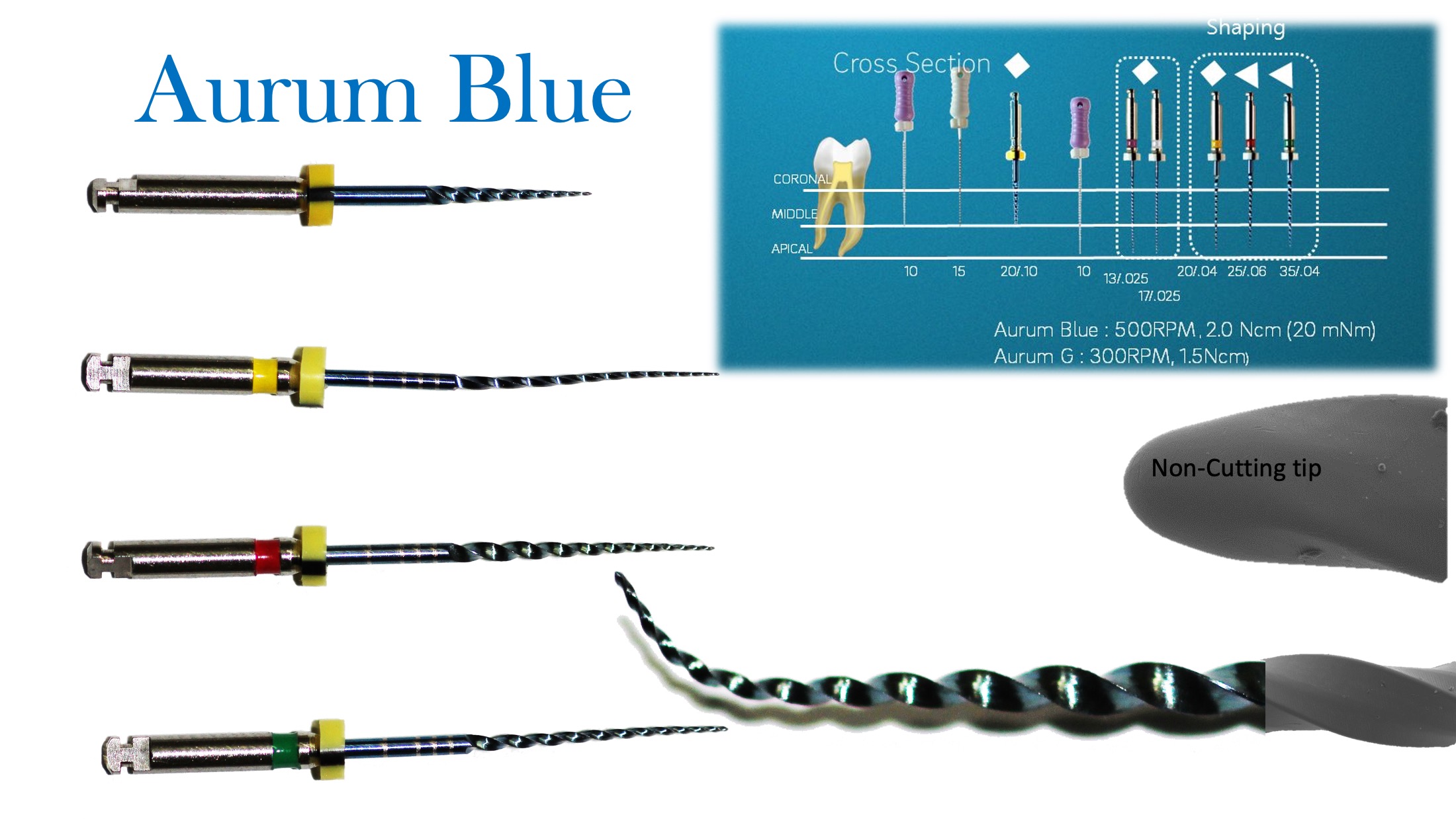
The use of endodontic files in the stabilised martensitic stage (controlled memory) will offer more resistance against cyclic fatigue.11, 13, 14 A calcium silicate-based endodontic sealer was sonically activated (CeraSeal and EQ-S, Meta Biomed) and gutta-percha was used to obturate the root canals (Figs. 8a–c). This stage of the treatment might be challenging when such a small endodontic access is created. The use of a calcium silicate-based endodontic sealer facilitates the obturation process, and the sonic activation helps to distribute the material all along the cleaned and shaped root canal system (Fig. 9). An adhesive coronal restoration was placed in the same appointment, a dual-polymerised core material (NexCore, Meta Biomed) for the pulp chamber and a compactable composite for the occlusal surface (Ezfil, Meta Biomed; Figs. 10a & b). The patient thereafter began orthodontic treatment, and the tooth was functional and the patient asymptomatic. The three-year follow-up radiograph showed healthy periapical tissue (Fig. 11).
Discussion
Fig. 12
Complications reported in autogenous transplantation cases include tooth fracture during extraction, root resorption, replacement resorption (rare), loose attachment, poor oral hygiene during the postoperative period and pulp necrosis (common), and root canal therapy will be necessary in most cases.15, 16 Among the advantages are that orthodontic movement will be possible, the procedure can be performed even in growing patients, and it offers the capacity to preserve the alveolar ridge and functional adaptation, which is very important in comparison with osseointegrated implants, which are stationary and do not erupt, resulting in infraocclusion in growing patients. One of the most cited advantages of this procedure is that typically a severely destroyed tooth can be exchanged for a tooth in perfect structural condition.4, 15, 17
Fig.13
When root canal therapy is necessary in the transplanted tooth, it is advisable to plan the treatment according to the status of the coronal and radicular structure. The preservation of the dental tissue should be a main goal, including the pursuit of minimally affected tooth resistance against occlusal load and functional stress. One of the greatest risks when performing conservative root canal therapy is that, while working through conservative access openings, the files will work under increased flexural stress; flexural stress will be higher at the entrance of the root canal owing to the lack of straight-line access. Cyclic fatigue might increase also at curvatures, leading to greater transportation and changing of original root canal anatomy. If cyclic fatigue is one of the major risks related to conservative endodontic openings, the use of files with enhanced cyclic fatigue resistance is advisable.18
Aurum Blue is a four-file root canal instrumentation system in the stable martensitic structural stage (Fig. 12). The cross section, taper, nickel–titanium alloy and electropolished surface treatment were designed and combined together to offer a good balance between cyclic and torsional fatigue resistance and high flexibility. All the files smaller than 25/.05 have a square cross section, and larger sizes have a convex triangular cross section. These files are recommended to be used at 500 rpm with 2 Ncm torque.
The CeraSeal calcium silicate endodontic sealer is a useful option for the use of the single-cone obturation technique (Fig. 13). This technique greatly facilitates the sealing of the root canal system when conservative endodontic procedures are performed. CeraSeal’s physical characteristics render it capable of providing a stable 3D seal,19–21 all without the need for vertical or lateral compaction procedures, whether warm or cold. The single-cone obturation technique can be used safely in combination with calcium silicate cements, owing to their physical and dimensional stability, good sealing properties, antibacterial potential, biocompatibility and bioactivity, being capable of stimulating periapical tissue repair.20–22 These materials are able to set in humid environments; this point is of major relevance considering the fact that dentine has a moisture content of approximately 20% and that working in moisture-saturated environments is a constant in the dental profession.20, 21, 23
Conclusion
Considering all the biological and functional advantages of autogenous transplantation of a tooth in comparison with an implant placement and all the possibilities of a minimally invasive approach to endodontic treatment using new technology applied to endodontic devices, files and sealers, autogenous transplantation may be a valid treatment alternative, especially in young and compliant patients.3
AUCKLAND, New Zealand: Social media increasingly shapes ideas about what constitutes a healthy, attractive or socially acceptable smile. Researchers from ...
TOKYO, Japan: Despite facing increasingly tight schedules and growing operational and financial pressures, today’s dental practitioners are expected to ...
AJMAN, UAE: Artificial intelligence (AI) is reshaping dental education by changing how students learn, educators teach and institutions prepare graduates ...

 Brazil / Brasil
Brazil / Brasil
 Canada / Canada
Canada / Canada
 Latin America / Latinoamérica
Latin America / Latinoamérica
 USA / USA
USA / USA
 Austria / Österreich
Austria / Österreich
 Bosnia and Herzegovina / Босна и Херцеговина
Bosnia and Herzegovina / Босна и Херцеговина
 Bulgaria / България
Bulgaria / България
 Croatia / Hrvatska
Croatia / Hrvatska
 Czech Republic & Slovakia / Česká republika & Slovensko
Czech Republic & Slovakia / Česká republika & Slovensko
 France / France
France / France
 Germany / Deutschland
Germany / Deutschland
 Greece / ΕΛΛΑΔΑ
Greece / ΕΛΛΑΔΑ
 Hungary / Hungary
Hungary / Hungary
 Italy / Italia
Italy / Italia
 Netherlands / Nederland
Netherlands / Nederland
 Nordic / Nordic
Nordic / Nordic
 Poland / Polska
Poland / Polska
 Portugal / Portugal
Portugal / Portugal
 Romania & Moldova / România & Moldova
Romania & Moldova / România & Moldova
 Slovenia / Slovenija
Slovenia / Slovenija
 Serbia & Montenegro / Србија и Црна Гора
Serbia & Montenegro / Србија и Црна Гора
 Spain / España
Spain / España
 Switzerland / Schweiz
Switzerland / Schweiz
 Turkey / Türkiye
Turkey / Türkiye
 UK & Ireland / UK & Ireland
UK & Ireland / UK & Ireland
 China / 中国
China / 中国
 India / भारत गणराज्य
India / भारत गणराज्य
 Pakistan / Pākistān
Pakistan / Pākistān
 Vietnam / Việt Nam
Vietnam / Việt Nam
 ASEAN / ASEAN
ASEAN / ASEAN
 Israel / מְדִינַת יִשְׂרָאֵל
Israel / מְדִינַת יִשְׂרָאֵל
 Algeria, Morocco & Tunisia / الجزائر والمغرب وتونس
Algeria, Morocco & Tunisia / الجزائر والمغرب وتونس
 Middle East / Middle East
Middle East / Middle East

 Dr. Cameron Shahbazian DMD MBARegister now1CELive webinar
Dr. Cameron Shahbazian DMD MBARegister now1CELive webinar
 Dr. Bruce McFarlane Certified Specialist in Orthodontics Fellow: Royal College of Dentists of Canada Diplomate: American Board of OrthodonticsLive webinar
Dr. Bruce McFarlane Certified Specialist in Orthodontics Fellow: Royal College of Dentists of Canada Diplomate: American Board of OrthodonticsLive webinar


 Prof. Dr. Wael Att, Dr. Andrea Laureti ITI Scholar Michigan, Dr. Acela MartinezLive webinar
Prof. Dr. Wael Att, Dr. Andrea Laureti ITI Scholar Michigan, Dr. Acela MartinezLive webinar
 Cat EdneyRegister now1CE
Cat EdneyRegister now1CE














 and after (b) splint removal.")




 and after (b) splint removal.")

 and just after nishing the endodontic access opening (b).")
, mesiobuccal (b) and distobuccal (c).")

 and after (b) removal of the isolation.")


 and just after nishing the endodontic access opening (b).")
, mesiobuccal (b) and distobuccal (c).")

 and after (b) removal of the isolation.")








To post a reply please login or register