Aesthetic medicine is increasingly taking on a global connotation of harmony and balance, defined certainly by historically evolved and shared canons, but progressively corresponding to a biopsychosocially functional profile.1 From this perspective, different practices find common grounds of expression, aimed primarily at the interdependence between structure and function, constituting a dynamic functional unit which possesses characteristic and integrative links.2 In this article, we will take a deeper look at the contributions of speech therapy to facial aesthetics3 and to the reorganisation of stomatognathic functions4 in synergy with aesthetic medicine and aesthetic dentistry5 and in response to the aesthetic patient, deeply interlinked with personal life experience—the most intimate emotions linked to the self and identity.6
The current state of affairs
Speech therapy deals with the physiopathology of human communication in its most diverse forms and, for reasons also of a practical nature, it has expanded its scope over time to various areas of intervention, including the study of oral functions.7 In this innovative evolution, the Conselho Federal de Fonoaudiologia (Brazilian federal council of speech therapy) has regulated the application of orofacial motility for aesthetic purposes,8 thus identifying a new possibility of use to evaluate, prevent and stabilise mimetic facial and/or cervical muscles, seeking the symmetry and harmony of the structures involved, with aesthetic results. Myofunctional intervention is considered a new objective of speech therapy intervention concerning aesthetics, with its own foundations and principles, and is aimed at the attenuation of expression lines that inevitably appear.3 This area naturally integrates with the typical skills and objectives of the established protocols of aesthetic medicine and aesthetic dentistry. In this regard, various authors have extensively studied the influence of dentofacial aspects on physical attractiveness and self-esteem, and they have clearly demonstrated how dental morphology and related aesthetics play a fundamental and decisive role in the perception of beauty and, indirectly, in the determination of the social success of an individual. The physical aspect, self-esteem and the ability to engage in interpersonal relationships are deeply interrelated. Therefore, it is possible to assert that facial structure, primarily that of the lower third of the face, has a great psychological and aesthetic impact and can certainly be more relevant than dental morphology alone.6
Ageing
Ageing is a process that causes an imbalance of homeostasis and greater vulnerability of the organism, as well as a reduced adaptation to environmental stimuli, and it affects cells, tissue and organs.9 Anatomically, ageing is determined by the multiple effects of the passage of time and the effect of gravity on the skin, soft tissue, and superficial and deep components of the face, and their mutual influences and volumetric alterations.10 Facial ageing is also determined by the interactions and relationship with the external environment of bones, muscles, ligaments and skin, especially the combined effects of gravity, bone resorption, decreased elasticity, loss and displacement of components, and superficial and deep subcutaneous fat.11 These relationships between tissue are mostly represented in the lower third of the face and the perioral area, so the study and treatment of these areas is of fundamental importance in aesthetic and anti-ageing practices concerning the face. In fact, the dislocation of panniculus adiposus related to the collapse of the superficial musculo-aponeurotic system (mimetic facial muscles) and reduced muscular tropism of the perioral area12 results in a substantial acceleration of chrono-ageing, which, being genetically determined and hormone-sensitive, remains difficult to approach directly. Also, the deterioration of these structures worsens the incidence of photoageing, which is mostly determined by the relationship of the individual with the external environment13 and his or her socio-existential habits (exposure to sun, diet, consumption of stimulants, physical activity, work, other lifestyle factors, etc.), making it difficult to control by professionals in its triggering components.14
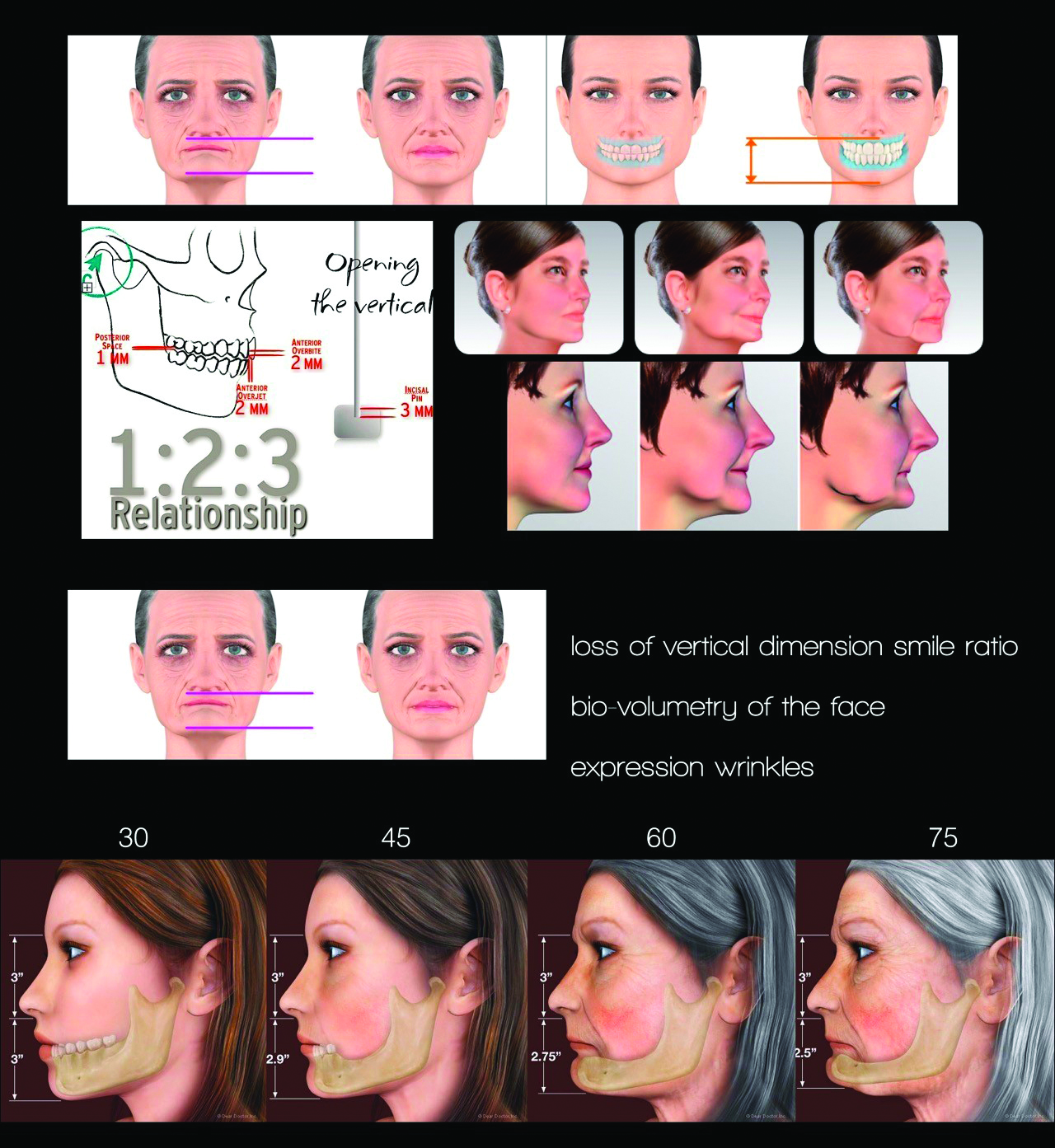
Fig. 1
Consequently, the study of the muscles of the lower third of the face and the related muscles and tissue changes becomes fundamental15 to physiological functions such as mastication, breathing, posture and facial expressions; to para-physiological conditions such as loss of vertical dimension (Fig. 1), collapse of the superficial musculo-aponeurotic system, preferential mastication, preferential sleeping side and chronic unilateral incidental sun exposure; and to pathological situations such as bruxism, previous injuries and trauma, loss of teeth or masticatory tissue, speech or language dysfunction, and disordered breathing.16 Just as the excessive contraction of the superficial mimetic muscles can promote the formation of wrinkles, so too can dysfunction of the stomatognathic system, consisting of a complex system of organs and tissue responsible for carrying out the respiratory, mastication, swallowing and communicative functions, cause chronic and repeated muscular contractions. The dysfunction of the respiratory, mastication and swallowing processes is characterised by a multifactorial aetiology and, with structural or functional involvement, is closely related to the expression lines on the sides of the mouth, thus resulting in specific postural attitudes. For these reasons, a single treatment is often ineffective. A synergistic approach between the dentist, speech therapist and aesthetic doctor addresses the problem with renewed therapeutic force, allowing better control of the formation of wrinkles and skin sagging and providing good mutual support in the clinical journey.
Dentistry and speech therapy
Several authors have demonstrated how effective a multidisciplinary vision and practical approach to the aesthetic clinical dentistry case are. In 2013, Bini proposed a facial aesthetic medical team (Fig. 2), a team of specialists that collaborate through a digital preview, an accurate multidisciplinary approach that has now been updated concerning aesthetics by providing for the involvement of speech therapy. The importance of the functional and aesthetic unit, such as the face and the smile, demands the most meticulous analysis of the harmony and beauty relationship, and the aesthetic patient, dysfunctional or not, must be motivated by this type of approach; without patient compliance, no prescription will be successful. The diagnostic and therapeutic process, as already well established and consolidated between orthodontists and speech therapists, must suggest the importance of orthodontic therapy for smile aesthetics related to increasing self-esteem in addition to the psychological and psychophysical well-being of the patient. The coordinated movements of all the orofacial muscles, as well as the posture of the tongue in the oral cavity, are essential for the physiological performance of the functions of breathing, mastication, swallowing and phonation, which is why in disease prevention and orthodontic therapy they are sometimes linked to facial aesthetic disharmonies. There is also a specific myofunctional intervention aimed at rebalancing oral function. From an early age, orofacial muscle imbalance contributes to the genesis of dental-skeletal abnormalities and the dysfunction of the temporomandibular joints, manifested above all by imbalances in adulthood. Therefore, the critical role that orthodontics plays should not be overlooked in adults as regards the most modern therapies characterised by digital design and therapeutic finalisation by means of clear aligners. This is so even when the clinical case has a more cosmetic purpose, such as minimal tooth movements intended for simple alignment of the parameters useful for improving the smile, that is, the possible modification of shapes and sizes of the post-orthodontic dental clinical crowns or simply the objective of conservative direct or indirect additive restorations. In this regard, clear aligners, aesthetic veneers, conservative additive restorations, prostheses and implant prostheses possess a series of features that characterise such treatment as an aesthetic approach.
Fig. 2
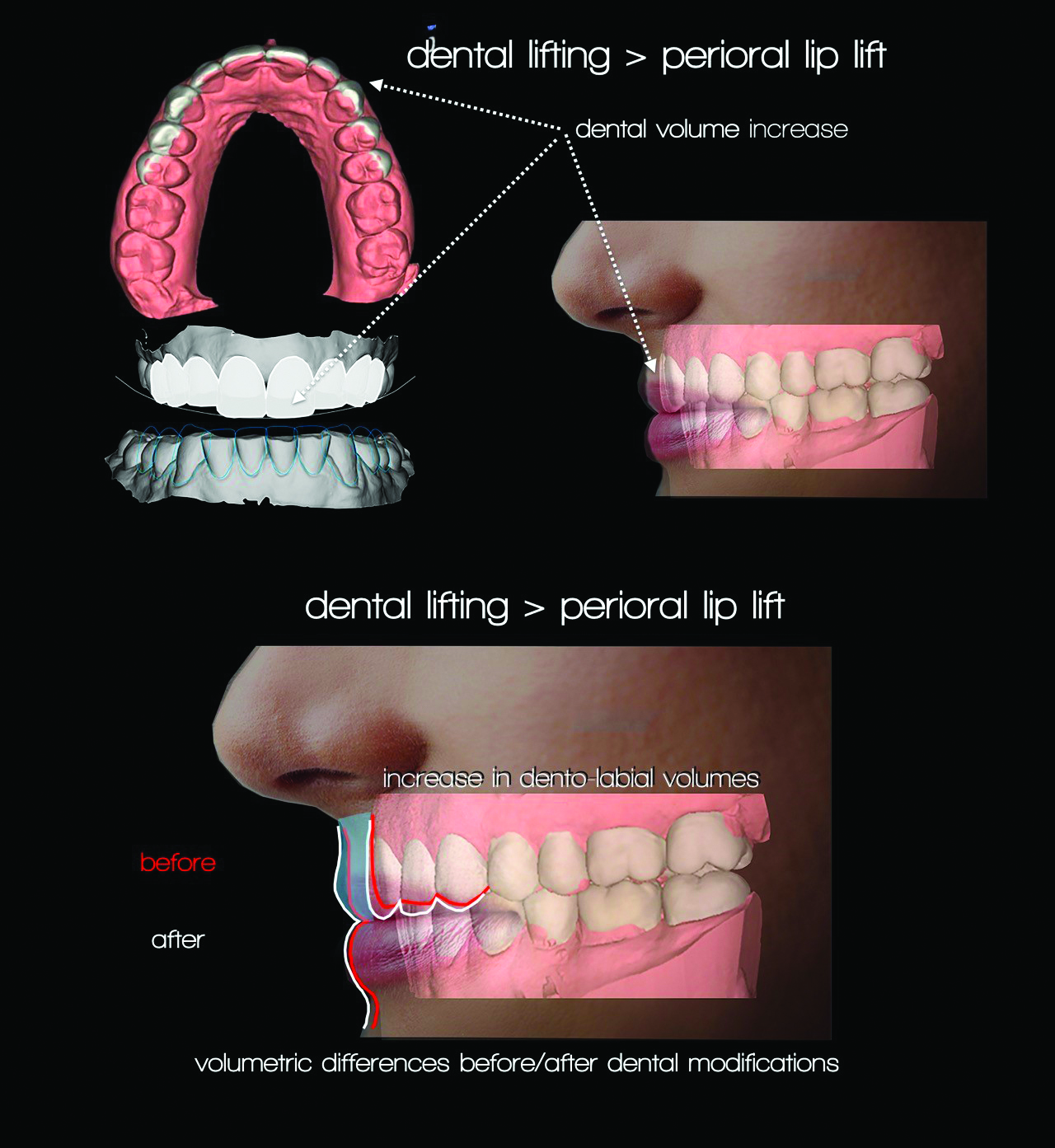
Fig. 3
Fig. 4
As a matter of fact, we must consider that any changes in positioning and volume of natural teeth and/or prostheses related to the 3D dimensions of other intra-oral tissue, such as bone and gingivae, can induce new bio-dimensional aesthetic such as stretching of vestibular tissue, increase of the vertical dimension with the consequent new dentolabial approach, and lifting of a lip induced by functional composition (Figs. 3 & 4), and phonetic and sublabial aesthetics related to dentistry. Static aesthetic analysis (photograph), dentolabial dynamics (video) and articulatory evaluation (audio) are decisive in the phase of consultation between the team’s specialists to be able to record any defects or functional and structural abnormalities in particular. It is essential to establish in a rational and economic manner the phases of the therapeutic process. Therefore, considering the aesthetic results, it will prove useful to foresee in the diagnostic stage any need for speech therapy before, during or after dental treatments.
The characteristics of the treatment process
In promoting facial harmony, which is understood as the highest degree of aesthetic and functional balance, it is essential to intercept the cause–effect relationship that exists between the equilibrium of the stomatognathic system, muscle function and the skin.17 Speech therapy intervention cannot be separated from an accurate initial multidisciplinary evaluation with the dentist and aesthetic doctor that is very often objectified through the use of digital images.6 High-resolution videos are essential, capturing the morphological and postural aspects of the following in a static and dynamic state: the face (posture, lips, tongue, dentition, occlusion, hard palate, soft palate, nostrils, eyes); tone (lips, tongue, cheeks, chin); proprioception; mobility (lips, tongue, jaw); stomatognathic functions (breathing, mastication, swallowing); facial symmetry; lifestyle habits; communication and eating habits.18 Based on the information gathered and the relationships observed between creases, wrinkles and oral imbalances, a personalized therapeutic process is proposed and articulated in different areas3 and can be treated directly within the dental practice (Fig. 5).
Fig. 5
Elongation and relaxation of the oral and perioral muscles through massage of the musculature (small massager roller and small vibrating device), and isometric and isotonic exercises derived from orofacial motility19
They act specifically on the different muscles of facial expression (orbicularis oris, levator labii superioris, levator labii superioris alaeque nasi, zygomaticus minor, levator anguli oris, zygomaticus major, risorius, buccinator, depressor anguli oris, depressor labii inferioris, mentalis, platysma, orbicularis oculi, occipitofrontalis, procerus, corrugator supercilii, nasalis). Massages, stretches and specific movements seem to promote increased blood circulation, tissue oxygenation, greater balance and muscular balance, and an increase in proprioceptive skills, all decisive in the reduction of the feeling of tension and fatigue.
Postural modification
Starting from the shared physical examination, we look for spontaneous labial occlusion, for the correct positioning of the lingual apex on the incisive papilla (in compliance with the relationships existing between structural and functional elements), and for postural balance in the head and neck region.
Rebalancing of stomatognathic functions
Through motor learning principles,20, 21 priority is given to nasal breathing,22, 23 bilateral alternating mastication,24, 25 functional swallowing26, 27 and balancing of temporomandibular joints.
Elimination of compensatory movements
Expressive mannerisms and dislocated tensions, possibly resulting from non-verbal communication, are normalised.28
The phases of intervention
The principle underlying treatment is the close connection between expression lines and orofacial muscle use over time. A structured course of action is therefore proposed,3 in consultation and integration with the dentist and aesthetic doctor, regarding the clinical process to be followed promptly:
Taking of a joint medical history (aesthetic doctor, aesthetic dentist, speech therapist) and evaluation of the stomatognathic system: Collaboration between the different specialists and the interdisciplinary vision, as well as the implementation of digital images processed by software such as Invisalign’s ClinCheck and Aesthetic Digital Smile Design,29 allows one to better individualise the treatment plan, which, thanks to the advent of digital dentistry, can create a standard result predictive of an optimal clinical outcome.
Holding of a session aimed at providing information on the proper functioning of the stomatognathic system and the structures involved.
Implementing of an intervention process of eight consecutive sessions, on a weekly basis, in which the patient acquires skills and autonomy in the daily performance of the different activities: In this regard, a daily work programme that the patient carries out independently for the duration of treatment is agreed on.
Holding of additional in-depth or control sessions.
Thanks to the stable acquisition of new skills, the patient will be able to proceed independently once the treatment process concludes.
Conclusion
The available literature on the clinical outcomes of different facial rejuvenation approaches through manipulation of the orofacial musculature is currently represented by single case reports and small case series and generally shows positive results.30–34 Isometric, static, dynamic exercises, massages, and specific manoeuvres seem to help prevent and reduce facial wrinkles. The following were specifically observed: reduction of wrinkles around the eyes, thinning of expression wrinkles, thinning of forehead wrinkles, volumetric and increased definition of the lips, increase in the tone of the cheeks, reduction of wrinkles on the neck, reduction of the nasolabial fold, increased skin tone, symmetry of the eyes, improved muscle tone, greater mandibular definition, adequacy of stomatognathic functions and attenuation of the signs of ageing. However, these positive findings must be interpreted in light of the procedures adopted for collecting the results, mainly based on self-assessment questionnaires and conclusive clinical evaluations,35 as well as in light of the very few clinical studies available which provide comparative pre- or post-treatment statistical data.32, 36
Therefore, a multidisciplinary intervention-based approach to the aesthetic patient seems even more promising. Such an approach can co-exist with proven mainstream approaches to aesthetic medicine and aesthetic dentistry. In conclusion, it remains essential to promote new interdisciplinary protocols between professionals in the three fields, under the direction of the dentist or aesthetic doctor, who, alongside the established aesthetic speech therapy-integrated solutions, can use this multidisciplinary approach to address facial ageing and promote the best degree of functional balance and aesthetic harmony. Thanks to the study of the new protocols proposed and further alternatives, it will be possible in the future to have a better statistical evaluation of the clinical evidence of the speech therapy approach in significant samples to enrich the current literature, in which this approach has been under-represented to date.
AUCKLAND, New Zealand: Social media increasingly shapes ideas about what constitutes a healthy, attractive or socially acceptable smile. Researchers from ...
TOKYO, Japan: Despite facing increasingly tight schedules and growing operational and financial pressures, today’s dental practitioners are expected to ...
AJMAN, UAE: Artificial intelligence (AI) is reshaping dental education by changing how students learn, educators teach and institutions prepare graduates ...

 Brazil / Brasil
Brazil / Brasil
 Canada / Canada
Canada / Canada
 Latin America / Latinoamérica
Latin America / Latinoamérica
 USA / USA
USA / USA
 Austria / Österreich
Austria / Österreich
 Bosnia and Herzegovina / Босна и Херцеговина
Bosnia and Herzegovina / Босна и Херцеговина
 Bulgaria / България
Bulgaria / България
 Croatia / Hrvatska
Croatia / Hrvatska
 Czech Republic & Slovakia / Česká republika & Slovensko
Czech Republic & Slovakia / Česká republika & Slovensko
 France / France
France / France
 Germany / Deutschland
Germany / Deutschland
 Greece / ΕΛΛΑΔΑ
Greece / ΕΛΛΑΔΑ
 Hungary / Hungary
Hungary / Hungary
 Italy / Italia
Italy / Italia
 Netherlands / Nederland
Netherlands / Nederland
 Nordic / Nordic
Nordic / Nordic
 Poland / Polska
Poland / Polska
 Portugal / Portugal
Portugal / Portugal
 Romania & Moldova / România & Moldova
Romania & Moldova / România & Moldova
 Slovenia / Slovenija
Slovenia / Slovenija
 Serbia & Montenegro / Србија и Црна Гора
Serbia & Montenegro / Србија и Црна Гора
 Spain / España
Spain / España
 Switzerland / Schweiz
Switzerland / Schweiz
 Turkey / Türkiye
Turkey / Türkiye
 UK & Ireland / UK & Ireland
UK & Ireland / UK & Ireland
 China / 中国
China / 中国
 India / भारत गणराज्य
India / भारत गणराज्य
 Pakistan / Pākistān
Pakistan / Pākistān
 Vietnam / Việt Nam
Vietnam / Việt Nam
 ASEAN / ASEAN
ASEAN / ASEAN
 Israel / מְדִינַת יִשְׂרָאֵל
Israel / מְדִינַת יִשְׂרָאֵל
 Algeria, Morocco & Tunisia / الجزائر والمغرب وتونس
Algeria, Morocco & Tunisia / الجزائر والمغرب وتونس
 Middle East / Middle East
Middle East / Middle East

 Dr. Cameron Shahbazian DMD MBARegister now1CELive webinar
Dr. Cameron Shahbazian DMD MBARegister now1CELive webinar
 Dr. Bruce McFarlane Certified Specialist in Orthodontics Fellow: Royal College of Dentists of Canada Diplomate: American Board of OrthodonticsLive webinar
Dr. Bruce McFarlane Certified Specialist in Orthodontics Fellow: Royal College of Dentists of Canada Diplomate: American Board of OrthodonticsLive webinar


 Prof. Dr. Wael Att, Dr. Andrea Laureti ITI Scholar Michigan, Dr. Acela MartinezLive webinar
Prof. Dr. Wael Att, Dr. Andrea Laureti ITI Scholar Michigan, Dr. Acela MartinezLive webinar
 Cat EdneyRegister now1CE
Cat EdneyRegister now1CE
























To post a reply please login or register