NEW YORK, U.S.: We, as dentists, have developed outstanding new technology in order to fashion beautiful smiles. The option to retain the natural dentition or replace it with implants opens limitless possibilities. As an endodontist, however, my mission is to preserve functioning teeth when possible. In the process, I focus on integrating the patient’s needs with technology. Today, advances in dentistry provide us with new choices when confronting the challenges of the past. Calcified canals are considered by many to be one of those challenges.
In fact, this condition frequently limits our ability to treat affected teeth. As we all know, leaving behind untreated, infected canals is a recipe for failure that may lead to extraction. Treating and saving nonvital roots with severe calcification challenges even the most talented practitioner. Various methods of bypassing calcification have been tried, but they frequently result in over-preparation or perforation. Let us take a look at a fresh approach to this old problem.
All treatment begins with a review of the chief complaint, a comprehensive examination, a review of the medical and dental history, diagnosis and treatment planning. It is important to note that not all calcified canals need root canal therapy. The foundation for endodontic treatment is based on the research performed by Kakehashi et al. Their findings established that endodontic care is indicated when there is bacterial contamination, leading to irreversible pulpitis or pulpal necrosis.
Not every problem requires reinventing the proverbial wheel. New use of existing technology may be the answer. For example, surgical templates assist implant placement. Their use for guidance through a calcified root is just a new application.
The process begins with taking a CBCT image to identify and visualize the root canals. CBCT, 3D imaging, frequently reveals canals not observable on 2D conventional periapical films. Examples include those elusive second mesiobuccal canals often missed in maxillary molars or second canals observed in mandibular incisors and premolars. When calcification of canals develops, it commonly starts in the chamber and travels apically. When a tooth undergoes calcific metamorphosis, the canals frequently are obscured from view in the coronal and middle thirds of the root but visible in the root’s apical third. When these canals are examined on the CBCT image, although not visible, a straight path may be imagined from the chamber to the canal in the root’s apical third. Computer software is now available to reproduce this path through the calcification to the remaining canal. SICAT Endo offers a service that streamlines the process.
After capturing the CBCT image, scan a digital impression of the same arch. Superimpose the data set of the digital impression over the data set of the CBCT image. Select four common points on both arches to align the information. Once matched and joined, the previously imagined pathway can be accurately measured from a cusp tip to the residual canal on the software. This digital information is ready to use to create a guide.
The next step is to use software to design a rigid template that fits over the occlusal or incisive surface. The template needs to extend beyond the treated tooth in both directions. This added dimension offers stability when seating the template. A space is designed in the template, over the tooth, to hold a 5 mm metal sleeve. On the computer, align the sleeve with the proposed pathway. Fabricate the template with a 3D printer. After it is created, insert the sleeve into the template. Drills that fit the sleeve’s internal diameter are selected based on the length needed to reach the residual canal. The guide is now complete and ready to use.
The measurement from the top of the sleeve to the viewable canal is determined on the computer. Access is gained through the guide with a low-speed handpiece. Once the residual canal is reached, treatment is completed following standard endodontic practices.
This approach reduces over-preparation of the canal and perforations. The dentist can apply a guide at any point during endodontic care. Each canal would require its own guide. The additional cost to the patient for fabricating the guide is much less than replacing the tooth. It enables predictable treatment of canals that otherwise would not be treatable. Very few patients have turned down the opportunity to save a tooth.
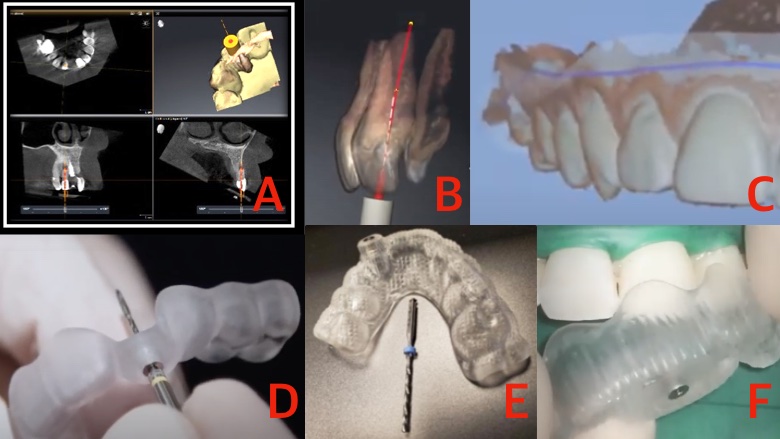
(A) Planning the guide path with CBCT software. (B) A planned path on the CBCT image. (C) An image of a digital impression in digital dentistry software. (D) An endodontic guide with a low-speed drill. (E) A template guide and drill. (F) Placing the guide over a tooth. (Images: Randolph Todd)
This example of the reapplication of technology may be useful in other areas of dentistry. The only limitation is our imagination. To provide a look into the future, I have listed other challenges we could pursue. I hope you read this with no expectations but rather an open mind for what could be.
Current technology: Patients have multiple electronic medical files containing history and current medications. In the future, DNA may also be available on a file.
Future potential applications: Fingerprint access or retinal scans could securely protect a single medical file that would efficiently transfer medical information to dentists. This information would enable personalized prescription of medications and more accurate use of the patient’s medical history. It may prevent accidental allergic reactions, adverse interactions and overprescribing.
Current technology: Microscopes can view computer screens through their optics.
Future potential applications: Radiographs, CBCT and digitalized impressions should be viewable through the microscope. The dentist could use tracked files (viewable on CBCT) in conjunction with preoperative or intraoperative images, to directly or indirectly guide the instrument, in an image-guided procedure.
Current technology: Ultrasonic light-activated nanoparticle-infused irrigation liquids need to be further adapted for irrigation of the canal system.
Potential dental application: Enhanced ultrasonic irrigation that would eliminate bacteria, viruses and prions.
Current technology: Laser fusion of dentin should be explored for obturation of root canals.
Potential dental application: The endodontic obturation process should seal the dentin and match the root’s physical properties to reestablish its strength. The process should be able to be reversed if retreatment is required.
Current technology: CBCT can identify canals and be used to measure their length accurately.
Potential dental application: This process should be automated.
The future may include significant advances in technology, but the application of existing technology will continue to open the doors for new treatment. Imagination is the key to unlocking those doors.
Up to now, the gold standard of obturation has been the continuous wave compaction technique.1,2 However, this technique is difficult to perform and needs ...
Much has changed in endodontics during the last 20 years, except the anatomy, which is still just as complex. We can improve our protocols and techniques, ...
DUNDEE, Scotland: Management of irreversible pulpitis in permanent teeth is undergoing a gradual but meaningful shift. Advances in diagnostic understanding ...
Periodontist and implant specialist Dr Lisa Heitz-Mayfield is very busy indeed. In addition to maintaining a specialist periodontics practice in West Perth ...
Implant dentistry has undergone a revolutionary transformation with the advent of digital workflows. These advancements have significantly improved the ...
The major causative role of micro-organisms in the pathogenesis of pulp and periapical diseases has clearly been demonstrated.[1] The main aim of endodontic...
VEVEY, Switzerland: Introduced by Swiss endodontic company Produits Dentaires (PD) at the 2019 International Dental Show, EssenSeal is an innovative sealer ...
Education
Live webinar Tue. 11 August 2026 1:00 pm EST (New York)
Artificial intelligence (AI) is moving rapidly from research and development into dental practice, raising important questions about implementation, ...
PRAGUE, Czech Republic: Alongside its prestigious scientific programme and international industry exhibition, the 2026 FDI World Dental Congress, which ...

 Brazil / Brasil
Brazil / Brasil
 Canada / Canada
Canada / Canada
 Latin America / Latinoamérica
Latin America / Latinoamérica
 USA / USA
USA / USA
 Austria / Österreich
Austria / Österreich
 Bosnia and Herzegovina / Босна и Херцеговина
Bosnia and Herzegovina / Босна и Херцеговина
 Bulgaria / България
Bulgaria / България
 Croatia / Hrvatska
Croatia / Hrvatska
 Czech Republic & Slovakia / Česká republika & Slovensko
Czech Republic & Slovakia / Česká republika & Slovensko
 France / France
France / France
 Germany / Deutschland
Germany / Deutschland
 Greece / ΕΛΛΑΔΑ
Greece / ΕΛΛΑΔΑ
 Hungary / Hungary
Hungary / Hungary
 Italy / Italia
Italy / Italia
 Netherlands / Nederland
Netherlands / Nederland
 Nordic / Nordic
Nordic / Nordic
 Poland / Polska
Poland / Polska
 Portugal / Portugal
Portugal / Portugal
 Romania & Moldova / România & Moldova
Romania & Moldova / România & Moldova
 Slovenia / Slovenija
Slovenia / Slovenija
 Serbia & Montenegro / Србија и Црна Гора
Serbia & Montenegro / Србија и Црна Гора
 Spain / España
Spain / España
 Switzerland / Schweiz
Switzerland / Schweiz
 Turkey / Türkiye
Turkey / Türkiye
 UK & Ireland / UK & Ireland
UK & Ireland / UK & Ireland
 China / 中国
China / 中国
 India / भारत गणराज्य
India / भारत गणराज्य
 Pakistan / Pākistān
Pakistan / Pākistān
 Vietnam / Việt Nam
Vietnam / Việt Nam
 ASEAN / ASEAN
ASEAN / ASEAN
 Israel / מְדִינַת יִשְׂרָאֵל
Israel / מְדִינַת יִשְׂרָאֵל
 Algeria, Morocco & Tunisia / الجزائر والمغرب وتونس
Algeria, Morocco & Tunisia / الجزائر والمغرب وتونس
 Middle East / Middle East
Middle East / Middle East

 Dr. Bruce McFarlane Certified Specialist in Orthodontics Fellow: Royal College of Dentists of Canada Diplomate: American Board of OrthodonticsLive webinar
Dr. Bruce McFarlane Certified Specialist in Orthodontics Fellow: Royal College of Dentists of Canada Diplomate: American Board of OrthodonticsLive webinar


 Prof. Dr. Wael Att, Dr. Kubra Kundak, Dr. Acela MartinezLive webinar
Prof. Dr. Wael Att, Dr. Kubra Kundak, Dr. Acela MartinezLive webinar
 Cat EdneyRegister now1CELive webinar
Cat EdneyRegister now1CELive webinar
 Dr. Allen Wong DDS, EdD, DABSCDRegister now1CE
Dr. Allen Wong DDS, EdD, DABSCDRegister now1CE





























To post a reply please login or register