The TADs are tied to the wire using a power chain looped to the wire, or NiTi closing springs, depending on the thickness of the tissue. (Images: Trevor S. Nichols & Stuart L. Frost)
As the profession of orthodontics evolves, we as orthodontists must continue to create solutions in order to offer a variety of treatment options to our patients. Furthermore, with the current challenges to our profession, we can elevate ourselves and our practices by expanding our possibilities and incorporating new treatment modalities. We must remember as specialists in orthodontics and craniofacial orthopaedics, every treatment plan should consider an orthodontic component, as well as an orthopaedic component, even in the non-growing patient. Remember, the word “orthopaedic” by definition means the correction of deformities of bones or muscles.1
Historically, these deformities were treated by surgery alone; however, with the advent of temporary anchorage devices (TADs), orthopaedic correction can be accomplished even in the non-growing individual. Since the introduction of TADs more than 35 years ago, Buschang et al. determined that more than half of the American Association of Orthodontists members surveyed had placed ten or fewer TADs and that the majority of orthodontists had referred the placement to another specialist.2 The purpose of this article is to explain and demonstrate simple TAD placement in routine orthodontic practice and suggest a few common uses for TADs.
TAD placement
For those new to TADs, or considering their use in practice, this section will describe a simple workflow for TAD placement that is repeatable and simple.
Step 1: Determine TAD location
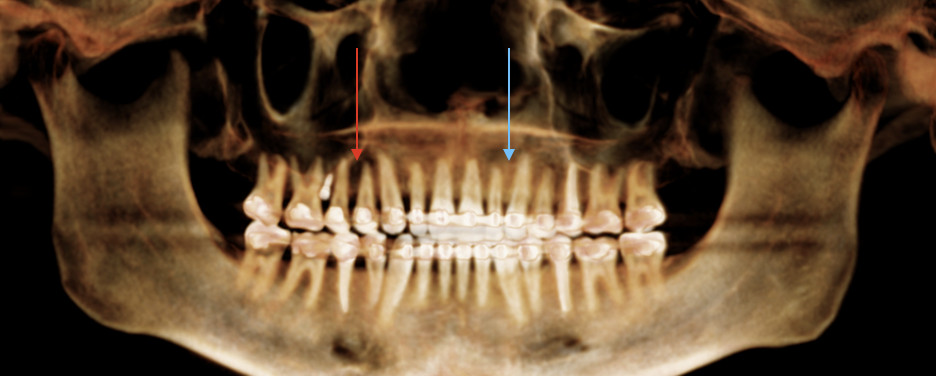
Fig. 1
Clearly, TAD placement will be determined in part by the mechanics they are used for. In addition to the mechanics used for TAD anchorage, there are important factors of individual anatomy that should be considered. A recent cone beam computed tomography scan, or panoramic radiograph, should first be obtained. This radiograph can be used to evaluate root divergence, bone height and, to some extent, bone density. Figure 1 demonstrates two areas indicated by both red and blue arrows. The red arrow indicates a radiolucent area, indicative of lower bone density. This would be an area where TAD placement would not be indicated. In contrast, the blue arrow indicates a radiopaque area, suggesting greater bone density and an area thus more ideal for TAD placement.
Step 2: Consider choices for anaesthesia
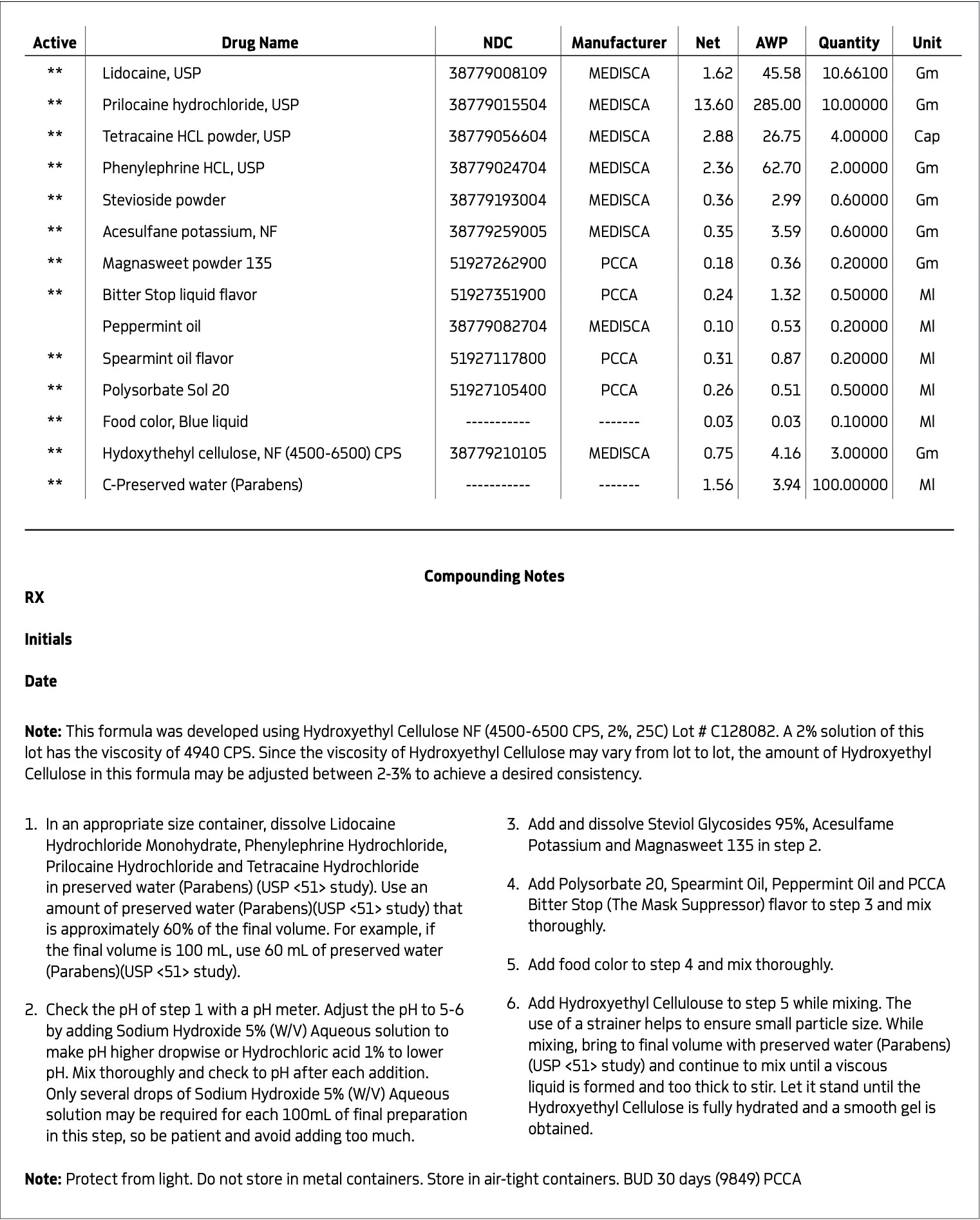
In our practice, we find that most patients prefer local anaesthesia (injection) for TAD placement, to ensure that they are comfortable during the procedure. For these cases, 2% lidocaine hydrochloride with 1:100,000 parts epinephrine is used via local administration, directly into the vestibule adjacent to the desired TAD location. Typically, one-quarter cartridge suffices to provide adequate anaesthesia. If the patient declines local anaesthesia, an alternative option used in our practice is a topical compound that is placed directly on the tissue (Fig. 2).
Fig. 2
Step 3: Hard- and soft-tissue clinical evaluation
Fig. 3
Once the TAD site has been located and the patient sufficiently anaesthetised, a clinical assessment of the hard and soft tissue is performed. For this assessment, a PKT2 waxing instrument (Hu-Friedy) is used. The waxing instrument is used first to verify anaesthesia. Then, a depression is made vertically, to mark the intra-radicular space. Next, the deepest area in the attached tissue is selected, approximately 1 mm occlusally, from the mucogingival junction, but not into the free mucosa. Using the vertical line and soft-tissue location, the waxing instrument is used to evaluate bone quality. This is done by pressing into the tissue and bone. If the bone feels solid, the site is selected. If the waxing instrument sinks into the bone, another location is selected along the intraradicular line (Fig. 3).
Step 4: TAD selection
Once the site is located, the appropriate TAD is selected. In our office, we use VectorTAS (Ormco). We use a 1.6 × 6.0 mm TAD in the anterior, a 1.6 × 8.0 mm TAD in the posterior and a 1.6 × 10.0 mm TAD for the palate. For buccal shelf, ramal and infra-zygomatic TAD placement, 2.0 × 12.0 mm stainless-steel bone screws (Ortho Bone Screw) are used.
Step 5: TAD placement
TADs are placed using either an electronic driver or a manual driver. We use the Orthonia driver (Rocky Mountain Orthodontics) alongside VectorTAS. Regardless of the method of insertion, a sturdy hand is important for TAD stability. Additionally, the clinician should feel the TAD going into the bone snugly. TAD is placed until the tissue blanches and the TAD neck is flush with the tissue.
Step 6: TAD verification
Once the TAD has been placed, a plier is used to verify primary stability. Because TADs do not osseointegrate, the day the TAD is placed is the most stable it will ever be. If primary stability is not obtained, remove and reinsert in another location using the same TAD on the day of initial placement. Ensure that Step 3 is repeated at the new TAD placement site prior to TAD placement. When considering the mechanics of TAD utilisation, anchorage can be divided into two categories. The first is direct anchorage, when the mini-screw or TAD is tied to a tooth with a spring, elastic or cantilever arm. The second is indirect anchorage, when a TAD is used and tied to another tooth, which is then used as anchorage.
Case 1: The gummy smile
One of the most common uses for TADs in our practice is to correct the gummy smile. This includes cases with absolute maxillary excess, posterior maxillary excess or anterior maxillary excess. These cases are all treated using TADs as direct anchorage for intrusion; they simply vary in location of intrusion.
Example 1:
The anterior gummy smile The anterior gummy smile is one in which the patient shows excess gingival display from maxillary canine to maxillary canine (Figs. 4 & 5, beginning of treatment). This takes into account the ideal crown shape and size, where the patient has true anterior maxillary excess and is not just in need of a gingivectomy or crown lengthening procedure. To best determine if gummy smile treatment is needed in the anterior, the authentic smile photograph is used, alongside measurement of the incisor display at rest. If the resting incisor display is greater than threequarters in the adult patient without altered passive eruption, gummy smile treatment is needed. These cases are treated using two TADs placed between tooth #13 and #12 or between #22 and #23 using a 1.6 × 6.0 mm TAD. If slight posterior impaction is desired, bite turbos with Triad Gel (Dentsply Sirona) are placed on teeth #37 and #47 and squeezing exercises used to impact posterior molars engaging the posterior fibres of the temporal muscles (60 squeezes six times per day).
Fig. 4
Fig. 5
Fig. 6
Fig. 7
Fig. 8
Fig. 9
Fig. 10
Fig. 11
Fig. 12
TADs are placed at the second visit with a 14 × 25 mm copper (Cu) and nickel–titanium (NiTi) wire and are tied from the anchor to the wire with an elastic thread (surgical thread; Fig. 6). Once the patient has progressed to larger Cu–NiTi wires and stainless steel, the TADs are tied to the wire using a power chain looped to the wire, or NiTi closing springs, depending on the thickness of the tissue (Figs. 7 & 8).
Once the intrusion has been completed, the TADs are tied to the wire and vertical elastics are used to close the bite without relapse of the intrusion. If buccal crown tip is seen, owing to the movement created by the intrusion, a power chain torquing sling is used to encourage lingual crown tipping and to prevent flaring of the incisors (Fig. 9). Once the case has been completed, the appliance is removed and a gingivectomy is performed to idealise the tissue shape and the final contours are made to the hard tissue (Figs. 10–12, end of treatment).
Example 2: Posterior gummy smile
The posterior gummy smile is a case in which there is posterior maxillary excess and the patient displays more than 4 mm of gingiva posteriorly (Figs. 13 & 14, beginning of treatment). For these cases, two posterior 1.6 × 8.0 mm TADs are placed between tooth #15 and #16 and between tooth #25 and #26 or between tooth #14 and #15 and between tooth #24 and #25. Bite turbos are placed on teeth #36 and #46 with Triad Gel to allow the lingual cusps of the maxillary molars to occlude with those of the mandibular posteriors to prevent buccal flaring of posterior teeth (Figs. 15 & 16).
Fig. 13
Fig. 14
Fig. 15
Fig. 16
Fig. 17
Fig. 18
Fig. 19
Fig. 20
Fig. 21
Fig. 22
Fig. 23
The same protocol is used, in which TADs are placed at the second visit with the 14 × 25 mm Cu–NiTi wire and tied to the archwire using elastic thread. Once in larger Cu–NiTi and stainless-steel wires, the TADs are tied to the wire using a power chain or NiTi closing springs (Figs. 17 & 18).
Once the impaction has been completed, the TADs are tied to the wire using steel ligatures and box elastics are used to close the posterior bite (Figs. 19 & 20). To maintain space closure, a tieback module is used from a hook on the mesial to the cuspid to the hook on the first molar and is placed occlusal to the brackets to prevent gingival impingement. Again, a gingivectomy is performed posttreatment to idealise tissue shape and size, and hardtissue contouring is performed (Figs. 21–23, end of treatment).
Example 3: Anterior/posterior gummy smile (the absolute gummy smile)
A case is considered an absolute gummy smile when there is absolute maxillary excess (Figs. 24 & 25, beginning of treatment). These cases combine the previously described methods, using a total of four TADs. Two anterior TADs are placed between tooth #12 and #13 and between tooth #22 and #23, two posterior TADs are placed between tooth #16 and #15 and between tooth #25 and #26 or between tooth #15 and #14 and between tooth #24 and #25, and bite turbos are placed on teeth #36 and #46 with Triad Gel (Fig. 26).
Fig. 24
Fig. 25
Fig. 26
Fig. 27
Fig. 28
Fig. 29
In some cases, intrusion may occur asymmetrically (one side faster than another, or the anterior faster than the posterior). For these occurrences, when one area has been completed with intrusion, the TAD is tied to the wire and intrusion continues in the others until all intrusion has been completed. A gingivectomy and hard-tissue contouring are completed (Figs. 27–29, end of treatment).
Case 2: Missing teeth
For various reasons, we commonly see missing teeth. Whether congenitally missing or extracted, it is nice to be able to offer various options to our patients, especially younger patients with congenitally missing posterior teeth. For many of these cases, we offer the solution of TAD placement and space closure with maximum anchorage.
Example 1: Missing teeth
For cases with missing teeth, TADs are placed anterior to the edentulous area, and used as indirect anchorage by tying with a stainless-steel ligature distal to the adjacent tooth (Figs. 30 & 31). A NiTi closing spring is then used to close the space. This is a simple and effective way to maintain anchorage and close space for missing teeth. Especially in cases with congenitally missing premolars, where the primary molar is not a long-term viable option, TADs are a great option in young patients to use as anchorage and close spaces by protraction.
Fig. 30
Fig. 31
Fig. 32
Fig. 33
Fig. 34
Fig. 35
Example 2: Missing premolars
The patient’s teeth are bonded initially, but the retained primary tooth is not bonded. Archwire progression is completed, and once the stainless-steel wire is placed, the retained primary teeth are extracted and TADs are placed mesial to the edentulous area and indirectly tied in order to use as anchorage. An NiTi closing spring is then used from a post on the archwire around the distal on the wire distal to the tooth just adjacent to the edentulous area. The space is then closed. A wire tie is placed to ensure space closure is maintained without continuous use of elastic chain (Figs. 32–35).
Case 3: Deep bite correction
Correction of severe deep bites can be challenging, particularly among adult brachycephalic individuals. For this reason, we supplement treatment with the use of TADs to aid in correction of the deep bite. If the mandibular canine to canine region needs intrusion, two TADs are placed and initially tied with elastic thread in light wires. Once stainless-steel wires are placed, a power chain is used to continue intrusion. If only mandibular incisors need intrusion, one TAD is placed in the midline to aid in correction.
Example 1: Deep bite intrusion of the mandibular canine to canine region in an adult
In cases where the deep bite consists of overeruption of teeth #43–33, two TADs are placed (1.6 × 6.0 mm) between tooth #42 and #43 and between tooth #32 and #33 to aid in opening the bite (Figs. 36–39).
Example 2: Deep bite intrusion of mandibular incisors in an adult
For deep bite cases in which just the mandibular incisors are extruded, a single TAD is placed between tooth #41 and #31 (Figs. 40 & 41).
Fig. 36
Fig. 37
Fig. 38
Fig. 39
Fig. 40
Fig. 41
Case 4: Mandibular distalisation
A great solution for Class III patients in need of mandibular distalisation for profile aesthetics and dental function is buccal shelf TADs. This solution allows for noncompliance correction of Class III cases with decreased compensation of the maxillary arch (Figs. 42–45, beginning of treatment). For these cases, a 2 × 12 mm Ortho Bone Screw is placed mesial to teeth #47 and #37 into the buccal shelf of the mandibular body. If the patient has mandibular third molars, then they are extracted right before the TADs are placed once in the stainless-steel wires.
Once the patient has progressed to stainless-steel wires, buccal shelf TADs are placed. A mandibular pre-posted stainless-steel wire is used, and a VectorTAS NiTi closing spring is placed from the buccal shelf TAD to the post (Fig. 46). Once the Class III has been corrected, a steel ligature is used to retain the Class III malocclusion while finishing and detailing are completed (Figs. 47–51, end of treatment).
Fig. 42
Fig. 43
Fig. 44
Fig. 45
Fig. 46
Fig. 47
Fig. 48
Fig. 49
Fig. 50
Fig. 51
Case 5: Skeletal expansion
In cases where absolute maxillary expansion is desired with little to no dental side effects, maxillary anchorage with TADs is a wonderful solution. This allows for sutural expansion that has little to no dental compensation. Many designs exist for TAD placement with expansion. In some cases, a tissue-borne expander is used with no anchorage on the molars. This is typically used to encourage the maximum amount of skeletal expansion when dental tipping is undesired (Figs. 52 & 53). In cases where molar anchorage is desired, a banded approach can be used in conjunction with TADs (Figs. 54–59).
Fig. 52
Fig. 53
Fig. 54
Fig. 55
Fig. 56
Fig. 57
Fig. 58
Fig. 59
Conclusion
For the orthodontist, TADs can change much of the way we practise. We can expand the way we change lives and impact our patients in a more profound way. TAD placement is simple and requires little clinical time. We recognize the pioneers in our industry who have made TAD use commonplace and thank them for their courage. The clinical uses for TADs are vast. Orthodontists should become comfortable with TAD placement and mechanics and should consider their use in various cases in clinical practice to help provide optimal treatment outcomes.
References
Lexico.com [Internet]. Oxford: Oxford University Press; 2020 [cited 2020 Aug 13). Available from: https://en.oxforddictionaries.com/definition/orthopedic.
Buschang PH, Carrillo R, Ozenbaugh B, Rossouw PE. 2008 survey of AAO members on miniscrew usage. J Clin Orthod. 2008 Sep;42(9):513–8.
PRAGUE, Czech Republic: The FDI World Dental Congress holds a special place in the annual dental calendar. This year’s edition will bring the global ...
MINNEAPOLIS, US: Despite recommendations to limit systemic antibiotic use for localised endodontic infections, prescribing in endodontic care remains an ...
LONDON, England: A ten-year analysis of National Health Service (NHS) dental prescribing in England suggests that antimicrobial and analgesic prescribing, ...
ANN ARBOR, Mich., US: Opioid overprescription remains a major concern in dentistry. Although the prescription of opioids by dentists in the US has decreased...
Antimicrobial resistance is a mounting global health threat, and dentistry accounts for a notable share of antibiotic use. In conflict-affected settings ...
LEEDS, England: While antibiotics remain essential for treating infectious diseases, their global efficacy is declining owing to the rise of antimicrobial ...
ANKARA, Turkey: It is well known that antibiotic resistance is a growing problem and that some bacteria have become resistant to even the most powerful ...
CORVALLIS, Ore., U.S.: The prescription of drugs in dentistry has recently been brought into question. Much of the discussion has been around opioids and ...
Education
Live webinar Thu. 6 August 2026 5:00 pm EST (New York)

 Brazil / Brasil
Brazil / Brasil
 Canada / Canada
Canada / Canada
 Latin America / Latinoamérica
Latin America / Latinoamérica
 USA / USA
USA / USA
 Austria / Österreich
Austria / Österreich
 Bosnia and Herzegovina / Босна и Херцеговина
Bosnia and Herzegovina / Босна и Херцеговина
 Bulgaria / България
Bulgaria / България
 Croatia / Hrvatska
Croatia / Hrvatska
 Czech Republic & Slovakia / Česká republika & Slovensko
Czech Republic & Slovakia / Česká republika & Slovensko
 France / France
France / France
 Germany / Deutschland
Germany / Deutschland
 Greece / ΕΛΛΑΔΑ
Greece / ΕΛΛΑΔΑ
 Hungary / Hungary
Hungary / Hungary
 Italy / Italia
Italy / Italia
 Netherlands / Nederland
Netherlands / Nederland
 Nordic / Nordic
Nordic / Nordic
 Poland / Polska
Poland / Polska
 Portugal / Portugal
Portugal / Portugal
 Romania & Moldova / România & Moldova
Romania & Moldova / România & Moldova
 Slovenia / Slovenija
Slovenia / Slovenija
 Serbia & Montenegro / Србија и Црна Гора
Serbia & Montenegro / Србија и Црна Гора
 Spain / España
Spain / España
 Switzerland / Schweiz
Switzerland / Schweiz
 Turkey / Türkiye
Turkey / Türkiye
 UK & Ireland / UK & Ireland
UK & Ireland / UK & Ireland
 China / 中国
China / 中国
 India / भारत गणराज्य
India / भारत गणराज्य
 Pakistan / Pākistān
Pakistan / Pākistān
 Vietnam / Việt Nam
Vietnam / Việt Nam
 ASEAN / ASEAN
ASEAN / ASEAN
 Israel / מְדִינַת יִשְׂרָאֵל
Israel / מְדִינַת יִשְׂרָאֵל
 Algeria, Morocco & Tunisia / الجزائر والمغرب وتونس
Algeria, Morocco & Tunisia / الجزائر والمغرب وتونس
 Middle East / Middle East
Middle East / Middle East

 Dr. Bruce McFarlane Certified Specialist in Orthodontics Fellow: Royal College of Dentists of Canada Diplomate: American Board of OrthodonticsLive webinar
Dr. Bruce McFarlane Certified Specialist in Orthodontics Fellow: Royal College of Dentists of Canada Diplomate: American Board of OrthodonticsLive webinar


 Prof. Dr. Wael Att, Dr. Kubra Kundak, Dr. Acela MartinezLive webinar
Prof. Dr. Wael Att, Dr. Kubra Kundak, Dr. Acela MartinezLive webinar
 Cat EdneyRegister now1CELive webinar
Cat EdneyRegister now1CELive webinar
 Dr. Allen Wong DDS, EdD, DABSCDRegister now1CE
Dr. Allen Wong DDS, EdD, DABSCDRegister now1CE










































































































































To post a reply please login or register