The co-editor-in-chief of the Journal of Adhesive Dentistry and chair of the Department of Oral Health Sciences at KU Leuven in Belgium, Prof. Bart Van Meerbeek, is one of the most respected authorities on the topic of dental bonding agents. In this interview, he discusses the latest generation of universal adhesives and details what he regards as the most important factors for long-term bond stability.
Prof. Bart Van Meerbeek is one of the most respected authorities on the topic of dental bonding agents. (Image: GC International)
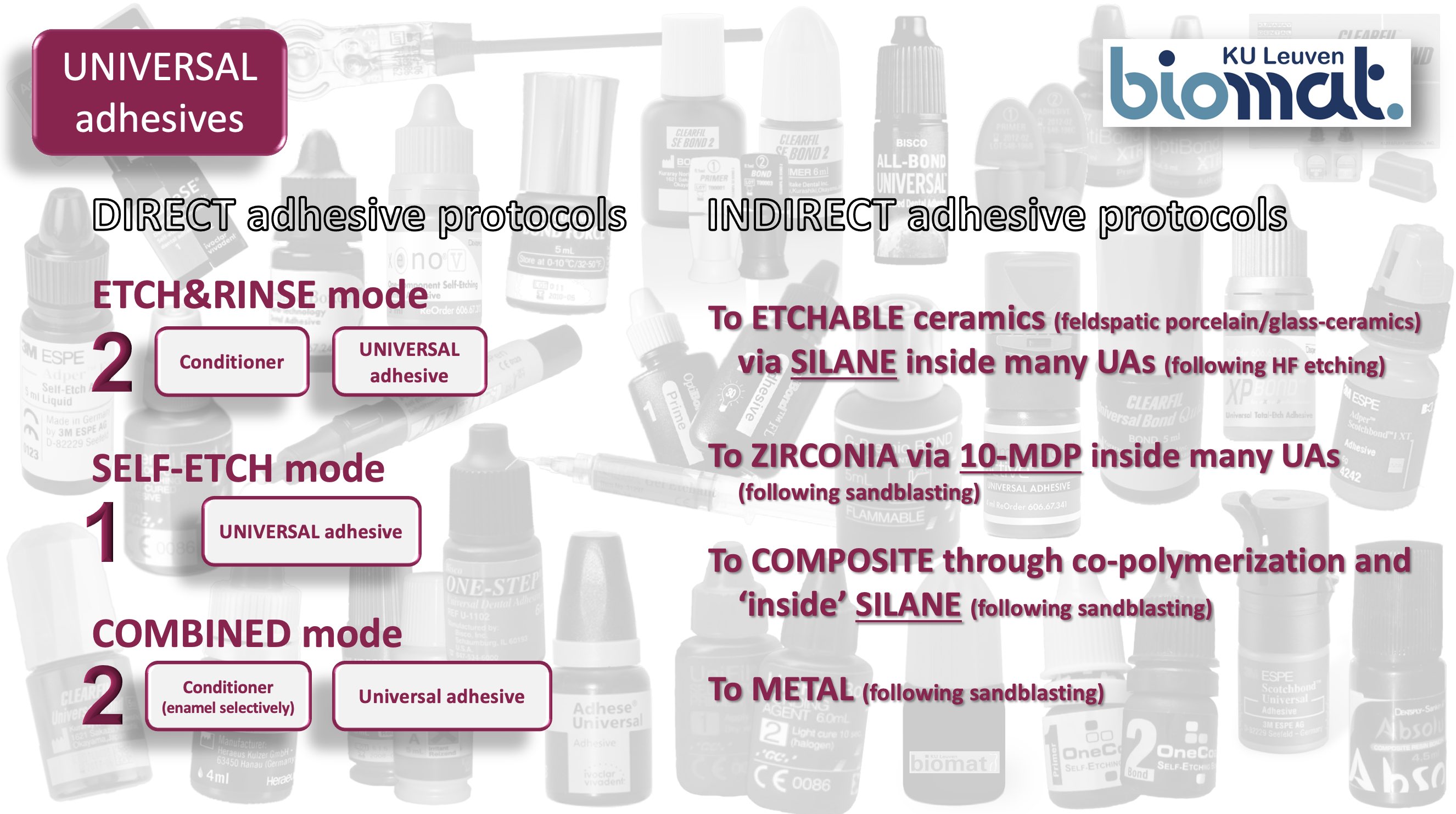
Prof. Van Meerbeek, the advantage of the simplified universal or multi-mode adhesives is that they unify etch-and-rinse (E & R) and self-etch (SE) modes. Despite the ongoing evolution of bonding agents, many dentists still opt for using one of the older generations of multistep adhesives. What do you think is the reason for that? Universal adhesives can indeed not only be used after E & R and SE bonding procedures, but they are also recommended for adhesive luting of indirect restorations. Some of them also contain silane in order to bond to glass ceramic, and most of them contain the MDP monomer (10-Methacryloyloxydecyl dihydrogen phosphate) to bond to zirconia, making it possible for this latest generation of adhesives to be used for both direct and indirect restorative procedures while being applicable in E & R, SE or selective-etch modes, hence the term “universal adhesive” (Fig. 1).
Despite all the advantages of universal adhesives, many dentists still prefer a certain type of bonding procedure or feel familiar with and are satisfied with a specific product; therefore, they do not see the need to change their bonding procedure and dental adhesive. In my opinion, what they were taught in their studies also contributes to their choice of bonding mode. Dentists tend to continue doing it that way, if they believe the technique that they have learned is efficient.
Personally speaking, when I use a universal adhesive, I follow a specific protocol for most of my clinical cases. My preference is the SE approach on dentine with selective etching of enamel beforehand, with exceptions for procedures such as bonding to hyper-mineralised and nearly impermeable sclerotic dentine. In such cases, I opt for the E & R approach.
Fig. 1: Direct and indirect adhesive protocols of universal adhesives. (Image: GC International)
For a long time, the scope of research was focused on the variety of adhesive monomers and the methodology of bond strength testing as well as the level of bond strength itself. Nowadays, the scope seems to be more on bond durability and long-term performance. How do you assess the different generations of bonding agents on that point? Firstly, I would like to emphasise that there is still a great deal of interest in the development of adhesive monomers. A good example of this is the number of R & D efforts to find a suitable replacement for 2-hydroxyethylmethacrylate (HEMA), which is still found in many adhesives, despite its numerous drawbacks. Another goal is to search for an equally effective but more hydrolytically stable successor of today’s most effective functional monomer, MDP.
Personally, I do not like the term “generation” to classify adhesives, as this does not describe the bonding mode that is employed for any particular generation of adhesives. I prefer referring to the two approaches, namely the SE and E & R bonding modes, and specifying the number of steps.
Most adhesives nowadays guarantee sufficient “immediate” bonding effectiveness, which means they perform well when bonded to model dentine in ideal laboratory circumstances and are tested relatively soon after application—usually after 24 hours or one week. Consequently, in most cases we cannot differentiate among today’s adhesives based purely on their immediate bond-strength data.
“The three-step E & R and two-step SE adhesives are still considered to be the gold standard”
For this reason, it is extremely important to challenge the products in order to learn their behaviour in the long term. As editor-in-chief of the Journal of Adhesive Dentistry, I must tell you that we do not accept papers reporting bond-strength data without ageing. Of course, artificial ageing in the laboratory cannot be directly translated to the clinical situation, but it at least provides an indication of the stability of the bond. I would recommend when testing adhesives to really challenge them by exposing specimens to long-term thermo-cycling (at least 50,000 cycles) or to immerse them in water for at least two months.
Though a scientifically documented product dependency exists, the three-step E & R and two-step SE adhesives are still considered to be the gold standard. This is mainly because sufficient and consistent evidence of favourable long-term bonding performance has been recorded for particular commercial adhesives in both laboratory and clinical research—the latter beyond ten years of clinical service. I believe all other simplified adhesives could be regarded as “trade-off” adhesives which have compromised some of their bonding performance for ease of use. For this reason, they have not yet reached gold standard levels and have also not been clinically tested for a sufficiently long period of time. For more details on this topic, see our opinion paper published in the Journalof Adhesive Dentistry (Fig. 2: Van Meerbeek et al. 2020; J Adhes Dent 22:7–34).
Fig. 2: Opinion paper on modern dental adhesive technology with plus/minus balances of the etch-and-rinse and self-etch modes. (Based on Van Meerbeek et al. 2020, with permission from Quintessence Publishing)
There are perceptions about a potential weakness of simplified E & R adhesives regarding collagen degradation and, for both E & R and SE approaches, regarding the hydrolysis of the polymer matrix itself. What is important for dental practitioners to know about these topics? Two main bond degradation pathways have been documented in the scientific literature. Firstly, there is the so-called enzymatic biodegradation, involving matrix metalloproteinases along with cysteine cathepsins. In the research, a great deal of attention has been focused on this pathway; however, the contribution of such enzymatic activity to bond degradation is still unclear and, in my personal opinion, much less relevant compared with the second bond degradation pathway. Secondly, there is water sorption or water uptake by the adhesive interface, inducing hydrolytic bond degradation mechanisms.
“The most important factor for bond durability is a stable and hydrophobic adhesive interface that ensures a good seal and prevents or limits water uptake”
I consider water sorption to be the most important degradation pathway. The oral environment and the dentine itself are the two water sources. The adhesive interface can absorb water from the underlying dentinal tissue through osmosis, especially when the adhesive is not cured right away. Together with water uptake from the outer oral environment, this may lead to hydrolytic degradation of the adhesive interface with dentine.
I believe that nowadays the importance of a good interfacial seal to prevent water sorption is underestimated. While this is besides the actual bonding performance, it is a primary requirement that an adhesive should meet. Too much attention is paid to enzymatic biodegradation, which I consider to be a research trend that will pass with time. In parallel, industrial R & D focuses on developing universal adhesives that combine primer and adhesive resins into single-solution formulations that proportionally contain less resin and more solvent, thereby making them more hydrophilic and consequently more sensitive to water sorption and thus to hydrolytic degradation.
The most important factor for bond durability is a stable and hydrophobic adhesive interface that ensures a good seal and prevents or limits water uptake. It must be made clear to general practitioners that adhesives should provide this minimally permeable seal.
Tooth erosion, bulk-fill techniques and shorter light-curing protocols—to mention just a few trends—create new challenges for adhesive dentistry. What are your recommendations in order to achieve a high level of bond strength, durability and long-term performance in direct protocols? My preferred bonding protocol combines selective enamel etching with an SE approach based on the MDP monomer. Among functional monomers, MDP is considered nowadays to be the most effective option available. On top of micromechanical interlocking achieved by the MDP monomer ’s etching capacity, this monomer provides additional chemical interaction potential. Chemical interaction is the innermost contact that molecules can have with one another, fundamental to bond durability. A common misunderstanding is the idea that chemical interaction will increase bond strength; it will not! Chemical interaction is only responsible for maintaining bond strength at a stable level.
Also of high importance for bond strength durability is the immediate seal of the interface. Postponing light curing creates osmotic effects with the consequence that water is absorbed from the underlying dentine. As mentioned earlier, this targeted interfacial seal must be, of course, highly hydrophobic.
I also strongly believe that in order to protect and stabilise the hybrid layer, the adhesive layer should have a certain thickness. A thick adhesive layer can act as a shock-absorbing layer or stress absorber that, for instance, compensates for the shrinkage of the layered composite and so will impose tensile stress to the underlying adhesive interface.
In summary, I would like to state that selective enamel etching, an SE approach based on the MDP monomer, a hydrophobic seal and an adhesive layer with a certain thickness are essential requirements in order to achieve long-term bond stability.
GC has a successful history in the development of HEMA-free bonding agents. What do you regard as the specific benefits of this feature? Today, HEMA is still added to many commercial adhesives owing to some of its positive features. It can act as a co-solvent for other monomers in preventing water/monomer phase separation. Thanks to its low molecular weight and thus small size, along with its high hydrophilicity, HEMA is an effective surface wetting agent as well as an interdiffusion/penetration agent. The latter feature enables it to infiltrate into the wet, demineralised collagen-rich dentine relatively deeply when exposed upon phosphoric acid etching as part of an E & R bonding protocol.
However, HEMA also has major disadvantages. It is too hydrophilic, and this leads to high water sorption. Universal adhesives contain water and HEMA in the same solution, and the fact that HEMA is so compatible with water makes it nearly impossible to remove water from the interface. Another negative point is HEMA’s low polymerisation ability, remaining soft and gel-like despite being cured. If it does not cure properly, the resin matrix will consequently not be strong enough. HEMA therefore contributes very little to the mechanical strength and stability of the polymer matrix. Another negative aspect is that, as it is a small molecule, it can compete with other functional monomers, inhibiting chemical interaction; for example, our research has shown that HEMA can affect the MDP monomer’s nano-layering. Its unfavourable biocompatibility, particularly in terms of its documented allergic potential, is also another disadvantage of HEMA that cannot be ignored.
Owing to all these limitations, dental manufacturers strive to develop and produce effective HEMA-poor/free adhesives, and there is definitely a need to find an effective replacement for HEMA.
“I believe, based on previous research, that a thicker adhesive layer can fulfil a stress/shock-absorbing function”
What would your wish list be for the most effective two-step bonding agent in terms of composition, technological features and performance? Selective enamel etching with phosphoric acid remains mandatory, unless a “universal” conditioner is discovered that creates sufficient micro-retention through etching enamel without depriving collagen from the protective mineral envelope. A separate primer should serve as adhesion promoter. This primer has to be MDP monomer-based, rendering chemical binding potential. This MDP monomer must be of good quality and be present in the solution in a sufficiently high concentration—at least 10% and up to 15%. The primer should also contain photoinitiators, not in order to allow the primer to be cured, of course, but in order to make sure that all areas, even in the deeper parts of the hybrid layer, will receive photoinitiators, so that the infiltrated resin can efficiently polymerise in situ after the adhesive resin in the third and final step is applied.
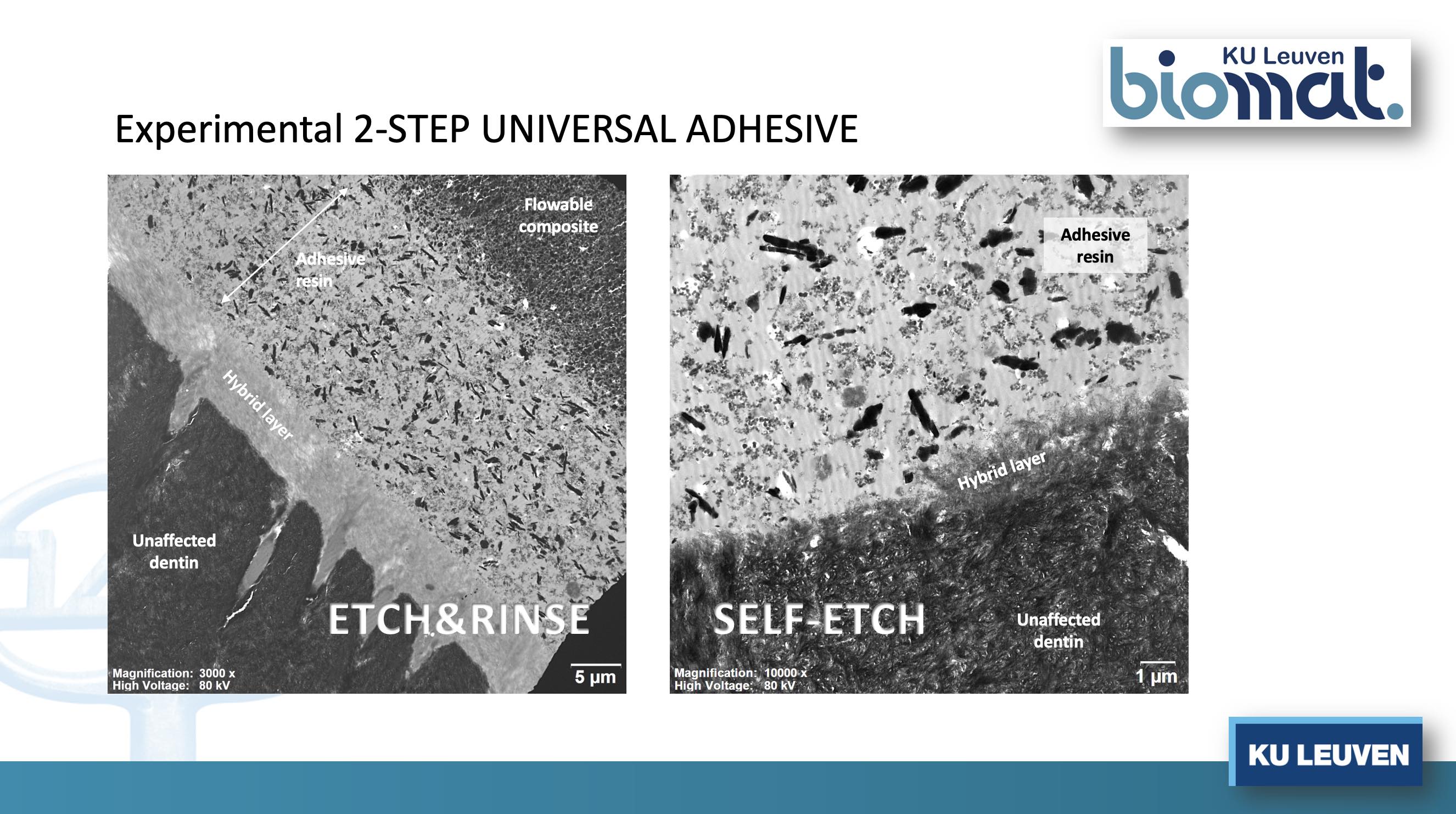
The final step involves the generous application of a separate adhesive resin, the actual glue. This adhesive should provide a good seal of the interface; it has to polymerise well, must present good mechanical properties and must be of hydrophobic nature to reduce water uptake. And it must be applied in a sufficiently thick layer (Fig. 3).
Fig. 3: Adhesive–dentine interface produced by an experimental two-step universal adhesive (precursor of the commercial adhesive G2-Bond Universal, GC) applied in etch-and-rinse and self-etch mode, typically exhibiting a relatively thick adhesive-resin layer with shock-absorbing potential (KU Leuven BIOMAT, 2020).
I believe, based on previous research, that a thicker adhesive layer can fulfil a stress/shock-absorbing function. When the composite that is placed on top of this layer shrinks, the interface is subjected to tensile stress; with an elastic layer (buffer layer), this tensile stress is prevented from causing interface de-bonding.
To conclude, this adhesive should be universal, in line with the current trend in dental adhesive technology, enabling its application in an E & R or SE bonding mode. It cannot be a trade-off, but should be an adhesive that can truly form a long-term stable bond with dentine and enamel.
In your opinion, would the application of a HEMA-free hydrophobic layer following the application of a hydrophilic primer optimise the adhesive performance to the tooth substrate? Dentin should always be properly sealed to prevent water from being absorbed by the adhesive interface through osmosis, which causes interfacial porosities and consequently weakens the interface. If sealed immediately, by the application of a HEMA-free hydrophobic layer, after correct polymerisation the water uptake is minimised, which reduces hydrolytic bond degradation over time. Hence, a multi-step universal adhesive is a logic next evolution.
1 thoughts on “Interview: “A multi-step universal adhesive is a logic next evolution””
In October last year, GC Holding announced the appointment of Dr Per Falk as CEO of the company. At the International Dental Show (IDS), Dental Tribune ...
The number of universal adhesives being offered by the dental industry nowadays can make it difficult to decide whether it may be worth switching to another...
COLOGNE, Germany: This morning, media representatives from around the world met at the Koelnmesse fairgrounds for the GC IDS press conference. The main ...
LUCERNE, Switzerland: G-CEM ONE is the newest self-adhesive resin cement from GC that simplifies procedures and brings together high bond strength, ...
LUCERNE, Switzerland: EQUIA Forte and EQUIA Forte HT, the glass hybrids from GC, are the ideal partners for dentists who want to practise environmentally ...
Through the Minamata Convention on Mercury in 2013, the countries of the EU committed themselves to completely or largely eliminating mercury-containing ...
Differences within material classes in CAD/CAM ceramics are not obvious at first glance. A knowledge of materials science is required in order to classify ...
Dr Andreas Kurbad established his private practice in Viersen in Germany in 1990 and started using CEREC in 1994. He has published more than 100 papers on ...
As pathological tooth wear becomes a more frequent concern in clinical practice, direct composite restorations are increasingly relevant as a minimally ...
Prof. Ivana Miletić from the Department of Endodontics and Restorative Dentistry at the University of Zagreb School of Dental Medicine in Croatia is one of...
LEUVEN, Belgium: GC Corporation is marking a special anniversary in the dental world this year as it looks back on 105 years of history. What began in 1921 ...
A metal–acrylic hybrid prosthesis has traditionally been a popular choice for implant-supported full-arch prostheses. More recently, zirconia has come to ...
TOKYO, Japan: Innovation in dentistry is often discussed in terms of new products; however, its clinical significance lies in how materials and technologies...

 Brazil / Brasil
Brazil / Brasil
 Canada / Canada
Canada / Canada
 Latin America / Latinoamérica
Latin America / Latinoamérica
 USA / USA
USA / USA
 Austria / Österreich
Austria / Österreich
 Bosnia and Herzegovina / Босна и Херцеговина
Bosnia and Herzegovina / Босна и Херцеговина
 Bulgaria / България
Bulgaria / България
 Croatia / Hrvatska
Croatia / Hrvatska
 Czech Republic & Slovakia / Česká republika & Slovensko
Czech Republic & Slovakia / Česká republika & Slovensko
 France / France
France / France
 Germany / Deutschland
Germany / Deutschland
 Greece / ΕΛΛΑΔΑ
Greece / ΕΛΛΑΔΑ
 Hungary / Hungary
Hungary / Hungary
 Italy / Italia
Italy / Italia
 Netherlands / Nederland
Netherlands / Nederland
 Nordic / Nordic
Nordic / Nordic
 Poland / Polska
Poland / Polska
 Portugal / Portugal
Portugal / Portugal
 Romania & Moldova / România & Moldova
Romania & Moldova / România & Moldova
 Slovenia / Slovenija
Slovenia / Slovenija
 Serbia & Montenegro / Србија и Црна Гора
Serbia & Montenegro / Србија и Црна Гора
 Spain / España
Spain / España
 Switzerland / Schweiz
Switzerland / Schweiz
 Turkey / Türkiye
Turkey / Türkiye
 UK & Ireland / UK & Ireland
UK & Ireland / UK & Ireland
 China / 中国
China / 中国
 India / भारत गणराज्य
India / भारत गणराज्य
 Pakistan / Pākistān
Pakistan / Pākistān
 Vietnam / Việt Nam
Vietnam / Việt Nam
 ASEAN / ASEAN
ASEAN / ASEAN
 Israel / מְדִינַת יִשְׂרָאֵל
Israel / מְדִינַת יִשְׂרָאֵל
 Algeria, Morocco & Tunisia / الجزائر والمغرب وتونس
Algeria, Morocco & Tunisia / الجزائر والمغرب وتونس
 Middle East / Middle East
Middle East / Middle East


 Dr. Crystal Marruganti, Cat EdneyRegister now1CELive webinar
Dr. Crystal Marruganti, Cat EdneyRegister now1CELive webinar
 Federico ZunicaRegister now1CELive webinar
Federico ZunicaRegister now1CELive webinar
 Dr. Sergio FlorencioLive webinar
Dr. Sergio FlorencioLive webinar
 Dr. Cameron Shahbazian DMD MBARegister now1CE
Dr. Cameron Shahbazian DMD MBARegister now1CE





















![Interview: “Glass hybrids […] are quite forgiving and tolerant regarding clinical challenges”](https://cdn.dental-tribune.com/dti//0001/00cd9fa6/cmVzaXplLWNyb3Aodz03NjY7aD00MDYpOnNoYXJwZW4obGV2ZWw9MCk6b3V0cHV0KGZvcm1hdD13ZWJwKQ/up/dt/2020/06/Interview-%E2%80%9CGlass-hybrids-%E2%80%A6-are-quite-forgiving-and-tolerant-regarding-clinical-challenges%E2%80%9D-1.jpg "Interview: “Glass hybrids […] are quite forgiving and tolerant regarding clinical challenges”")















Excellent overview of the evolution of adhesive bonding agents